

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Mineral trioxide aggregate (MTA) is widely used in endodontics since its introduction as root-end filling material of apical surgery.1 MTA is a hydrophilic powder that hydrates to form hydrated calcium silica and calcium hydroxide.2 MTA is now widely used in direct pulp capping and pulpotomy due to its sealing ability, antibacterial activity and biocompatibility.34 And MTA was used as apical barrier in root canals with open apex.5 Furthermore, MTA is used in the treatment of immature permanent teeth with necrotic pulp.56 Apexification or regenerative endodontics using MTA was reported. Resolution of periapical inflammation and continued root development was examined by regenerative endodontics.78
However, MTA should be removed and the teeth should receive conventional root canal treatment when periapical lesion is not healed in recall radiographs or root development does not progress after regenerative endodontics.69 Discoloration is often a problem especially in the case of anterior teeth after use of MTA.10 But the removal of set MTA is very challenging. MTA filled within root canal was not completely removed by using ultrasonics or rotary Ni-Ti instruments.11 Several studies evaluated whether acidic solutions affect physical properties of MTA.12131415 Microhardness and push-out strength or compressive strength of ProRoot MTA (Dentsply Tulsa Dental, Johnson City, TN, USA) were reduced by acidic solutions.121314 17% ethylenediaminetetraacetic acid (EDTA) inhibited hydration reaction of ProRoot MTA.16 10% citric acid (CA) reduced the microhardness of set Angelus MTA,15 whereas acidic solutions induced dentin erosion, decalcification.1517 Acidic solutions applied for short duration can dissolve the MTA.
Glycolic acid (GA) comes from fruit acids that are often called alpha-hydroxy acids. It is a retarder of hydration of portland cement and brushite,1819 and constituent of concrete remover.20 Therefore, GA could be useful as a MTA dissolving solution. However, its biocompatibility should be evaluated for use in the root canal.
OrthoMTA (BioMTA, Seoul, Korea) was developed for orthograde root canal filling material. OrthoMTA contains less heavy metals than ProRoot MTA (Dentsply, Tulsa, OK, USA),21 and was used as root canal filling materials in previous studies.2223 It was shown that intratubular mineralization of root canal dentin at the interface of dentin and obturated OrthoMTA by scanning electron microscope (SEM).2223 There has been no study about erosive effect of acidic solutions on the OrthoMTA.
In this study, therefore, the effect of 10% CA, 5% GA, and 17% EDTA on the surface microhardness of set OrthoMTA and root dentin was assessed. Also erosive effect of those solutions on OrthoMTA and dentin was assessed by SEM examination. In addition, the cytotoxicity of test solutions was evaluated using murine macrophage and WST-8 assay.
Materials and Methods
Specimen preparation
Study approval was obtained from the Institutional Review Board (IRB) of Seoul National University Dental Hospital (ERI 12006), Seoul, Korea. Forty extracted human single roots with single root canal were decoronated and 5 mm thickness dentin blocks, in the middle third of roots, were obtained using a diamond disc under continuous water irrigation. Root canals were prepared with size 2 through 6 Gates-Glidden burs (Dentsply Maillefer, Ballaigues, Switzerland) to form 1.5 mm diameter cavities, and irrigated with distilled water. After canal preparation, root canals were irrigated with 5 mL of 17% EDTA, 5 mL of 3.5% NaOCl to remove the smear layer.24 Finally canals were rinsed with 10 mL of distilled water. OrthoMTA powder was mixed with distilled water at a powder to liquid ratio of 3:1. The paste was packed into the dentin block using an amalgam carrier and OrthoMTA plugger (BioMTA) with a 1.0 mm sized tip. OrthoMTA was compacted using butt end of paper points with minimal pressure. Phosphate-buffered saline soaked gauze was placed on the top and bottom of the condensed OrthoMTA. Specimens were stored in an incubator with 100% humidity at 37℃. After 3 weeks, set OrthoMTA-dentin specimens were wet polished using silicon carbide sandpaper with decreasing particle sizes of 400, 600, 800, and 1,200 grit, respectively.
Microhardness test
Specimens were divided into four groups and exposed to one of following solutions for 5 minutes: 10% CA, 5% GA, 17% EDTA and saline (control) (n = 10). Specimens were wet polished with sand paper after exposure to solutions and then air-dried gently. The Vickers surface microhardness of Ortho MTA and dentin was measured before and after exposure to each solution with a HMV-2 microhardness tester (Shimadzu, Kyoto, Japan) and a square-based pyramid-shaped diamond indenter that produced a quadrangular depression with two equal orthogonal diagonals in the polished surface of the object. The angle between the opposite faces of the diamond indenter was 136 degrees. Microhardness test of dentin was performed at 0.5 mm level from canal lumen with full load of 200 g for 10 seconds at room temperature. Microhardness test of OrthoMTA was done at 25 g for 5 seconds. The Vickers microhardness value was displayed on the digital readout of the microhardness tester. Three indentations were made on the polished surface of each specimen that were more than 1 mm or more apart from each other. The mean value of the three measurements was calculated to determine the microhardness value for each specimen. Differences between microhardness values of OrthoMTA and dentin exposed to the four different solutions were analyzed with 1-way ANOVA followed by Tukey's post hoc test. Mean change in microhardness values of OrthoMTA and dentin within the groups were compared with student t-test. Statistical analysis was done with IBM SPSS version 23 software package (IBM Corp., Armonk, NY, USA) with a level of significance set at p = 0.05.
SEM examination
For the morphological evaluation of the root canal lumen dentin, other twelve specimens were prepared as described above. OrthoMTA was filled within dentin blocks of 1.5 mm diameter and 5 mm height. Specimens were stored in an incubator for 3 weeks. Subsequently, filled OrthoMTA was retrieved with size 140 K-files under irrigation. Irrigation was carried out with one of the following solutions, 10% CA, 5% GA, 17% EDTA, and saline for three specimens each respectively. Ten mL of solution was delivered in a syringe with 25-gauge needle to each root. Total irrigation time was about 5 minutes for each root. Then, the root canals were finally flushed with 10 mL of distilled water. The roots were split in half by creating two longitudinal grooves on their outer surfaces using a low-speed diamond disc (NTI, Kahla, Germany), avoiding penetration into root canals. The roots were then split along their long axis using a hammer and #15 surgical blade. The split roots were sectioned longitudinally to examine erosion of dentinal tubules of the root canal lumen. The split roots were mounted on aluminum stubs, sputter-coated with a 30 nm layer gold, and examined by FE-SEM (S-4700, Hitachi, Tokyo, Japan) to assess dentinal erosion. The voltage was set to 15.0 kV, the signal type was secondary electrons, and the working distance was 13 mm.
In addition, microstructure of the OrthoMTA surface exposed to test solutions was examined by FE-SEM. OrthoMTA powder was mixed with distilled water at a powder to liquid ratio of 3:1. Eight disc specimens of 2 mm diameter and 5 mm height were prepared using polycarbonate cylindrical molds. The OrthoMTA specimens were covered by distilled water-moistened gauze, stored in an incubator with 100% humidity at 37℃. After 3 weeks, the OrthoMTA specimens were exposed to one of the following solutions for five minutes- saline, 10% CA, 5% GA, 17% EDTA, each of two specimens. Then, the specimens were air-dried, mounted on aluminum stubs, sputter-coated with a 30 nm layer gold, and examined by FE-SEM (S-4700, Hitachi). Additionally energy dispersive spectroscopy (EDS) analysis was performed.
Cytotoxicity test
To compare cytotoxic effects of 10% citric acid, 5% glycolic acid and 17% EDTA, cell viability assay was performed on murine macrophage. Medium and reagents for cell culture were purchased from GIBCO-BRL (Life Technologies Inc., Grand Island, NY, USA). Murine macrophage cell line RAW 264.7, obtained from the American Type Culture Collection (ATCC, Rockville, MD, USA), was cultured in Dulbecco modified Eagle medium (DMEM), supplemented with 4.5 g/L glucose, 10% fetal bovine serum (FBS), and antibiotic solution (100 U/mL of penicillin-G and 100 µg/mL of streptomycin). Cultures were incubated at 37℃ in a humidified atmosphere of 5% CO2.
Each experiment was conducted using three cultures for each group. Experimental groups were: ① negative control, fresh DMEM culture medium, ② positive control, DMEM medium containing 0.1% zinc diethyldithiocarbamate (ZDEC), ③MEM culture medium containing 10% CA solution diluted to 1.0, 0.5, 0.2, 0.1%, ④ DMEM culture medium containing 5% GA solution diluted to 1.0, 0.5, 0.2, 0.1%, ⑤ DMEM culture medium containing 17% EDTA solution diluted to 1.0, 0.5, 0.2, 0.1%, ⑥ DMEM culture medium containing saline diluted to 1.0, 0.5, 0.2, 0.1%. Cytotoxicity of the test solutions was evaluated after 24 hours incubation period. After aspiration of culture supernatants, macrophage viability was measured with a Cell Counting Kit-8 (WST-8, Dojindo Laboratories, Gumamoto, Japan). RAW 264.7 cells were replenished with 100 µL culture medium (without phenol red) containing 10% WST-8. After incubation for 1 hour at 37℃ in a humidified atmosphere (5% CO2/95% air), optical density of the reacted suspension was directly measured at 450 nm by using an automated plate reader (Sunrise, TECAN, Salzburg, Austria). Statistical analysis was conducted with 1-way ANOVA of variance, followed by Tukey post hoc test to identify differences among the groups in the cytotoxicity test.
Results
Microhardness test results
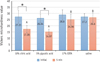
The results of microhardness tests are shown in Figures 1 and 2. Initial (pre-treated) microhardness values of set OrthoMTA or dentin were not different significantly amongst the four groups. Post-treatment microhardness test results of OrthoMTA showed that saline group (26.60 N/mm2) had the highest microhardness value followed, in descending order, by EDTA group (24.96 N/mm2), CA group (17.28 N/mm2), and GA group (14.97 N/mm2). Five minute exposure of 10% CA and 5% GA significantly reduced microhardness of set OrthoMTA than 17% EDTA or saline (p < 0.001, Figure 1). Microhardness value of OrthoMTA treated by 10% CA group and 5% GA group were not significantly different (p > 0.05).
Post-treatment microhardness test results of dentin showed that saline group (48.87 N/mm2) had the highest microhardness value followed, in descending order, by GA group (42.05 N/mm2), CA group (40.80 N/mm2), and EDTA group (35.46 N/mm2). Five minute exposure of 5% GA, 10% CA, and 17% EDTA significantly reduced microhardness of dentin than saline group (p < 0.05, Figure 2), whereas 17% EDTA significantly reduced the dentinal microhardness compared to 10% CA (p = 0.034) or 5% GA (p = 0.006).
SEM examination
Saline-treated dentin showed no dentinal erosion. Abundant collagen fibril network was identified by SEM (Figures 3a and 3b). Erosion of dentin was observed in the 10% CA or 17% EDTA-treated specimens. Dentinal tubules widened and collagen was extremely collapsed (Figures 3d and 3f), whereas, erosion with slightly widened dentinal tubules was only identified in the 5% GA-treated dentin (Figure 3h).
Microstructure of OrthoMTA is shown in Figure 4. Saline-treated OrthoMTA demonstrated abundant globular crystals (Figures 4a - 4c). The surface of OrthoMTA etched by 10% CA or 5% GA demonstrated destruction of matrix (Figures 4d - 4i). No apparent cubic crystal was seen in the citric acid treated OrthoMTA. A few needle-like and laminated crystals with loss of matrix are identified (Figures 4d - 4f). In the GA treated OrthoMTA, microchannels were seen with loss of matrix. Cubic crystal was destructed (Figures 4g - 4i). At the surface of 17% EDTA exposed OrthoMTA, partial erosion of the cubic crystals were noticed (Figures 4j - 4l). EDS analysis indicated that calcium content was lower in the CA or GA treated specimens than the saline treated specimens.
Cytotoxicity test
Cellular viability of 4 different test solutions at 0.1% dilution was not significantly different (p > 0.05). However, EDTA solution exhibited significantly more cellular cytotoxicity than CA and GA at 0.2, 0.5, and 1.0% diluted concentrations (p < 0.05, Figure 5). The cytotoxicity of CA and GA was slightly more than that of saline at 0.5 and 1.0% diluted concentrations (p > 0.05), without significant difference from each other.
Discussion
Microhardness measurement could provide indirect evidence of mineral loss in dental hard tissues.25 Dentin hardness is related to location. Its value decreases when the hardness test is made closer to the pulp, as tubular density increases.26 In this study, the microhardness measurement was obtained from three indentations located at 0.5 mm away from the canal lumen of coronal side of dentin disc, in order to control variables of tubule density. In the present study the measurements of microhardness of set OrthoMTA, with or without a given test solution were not performed on the same surface of samples. Because the diameter of OrthoMTA, filled within dentin disc was 1.5 mm, three microhardness indentations were possible on one side of set OrthoMTA, located 1 mm apart from each other. Thus microhardness test of set OrthoMTA was made on one side before exposure, and the other side after exposure to test solutions.
EDTA and CA have been used as root canal chelating agents.27 Erosion of dentin by CA or EDTA has been shown, in accordance with previous studies.2829 17% EDTA had the greatest effect on dentin in the present study. Likewise, 17% EDTA induced more calcium dissolution than 10% CA.17 Calt and Serper suggest that one minute application of 17% EDTA was effective to remove the smear layer.30 But previous studies evaluated the effect of root canal irrigants on the microhardness of the root canal dentin for five minutes.2831 Likewise, the present study used test solutions for 5 minutes. But erosion of OrthoMTA for five minutes would not sufficiently weaken the OrthoMTA surface to retrieve it. Therefore, elongation of exposure time to ten or twenty minutes would be beneficial in order to provide clinical relevance.
In this study, 5% GA and 10% CA significantly reduced microhardness of set OrthoMTA. There was a negative correlation between solubility and microhardness of restorative materials.32 Reduction of microhardness of OrthoMTA possibly indicate that OrthoMTA could be dissolved by acidic solutions. As surface microhardness decreased, deeper region of MTA would be exposed to acidic solutions. Moreover, structural change of OrthoMTA was induced by the contact of acidic solutions. Large voids and porosities were identified by SEM (Figure 4). Consequently, integrity of MTA cement was lost which would result in improvement of MTA retrieval by ultrasonic tip or files.
5% GA and 10% CA are organic acid, with pH of 2.11 and 1.59, respectively at room temperature. Matrix loss was examined by SEM of the acid-etched surface of ProRoot MTA by 37% phosphoric acid.14 OrthoMTA is mainly composed of tricalcium silicate, dicalcium silicate, bismuth oxide, and 5% of calcium carbonate according to the manufacturer. The inherent calcium carbonate was possibly soluble in acidic solutions and contributed to the dissolution of OrthoMTA. In addition, hydration product of OrthoMTA possibly interacted with carbon dioxide in the air during the dissolution process.33 When MTA is hydrated, calcium-silicate hydrate gel and calcium hydroxide is formed.34 Calcium ion of the calcium-silicate hydrate or calcium hydroxide interacts with carbon dioxide. Consequently, calcium carbonate is formed, which is called carbonation, and set OrthoMTA was dissolved in this study. Globular cubic crystal was identified in the SEM photographs of saline treated OrthoMTA (Figure 4c). While acid-etched OrthoMTA surface demonstrated that cubic crystals were destructed (Figures 4f and 4i). The cubic crystal was assumed to be calcium carbonate. The calcium carbonate crystal was dissolved by acid to be amorphous. Concentration of carbon dioxide of exhaled breath is about 5%, higher than that in the air. Carbonation of the calcium-silicate hydrate or calcium hydroxide would occur more frequently during root canal treatment than this in vitro experiment. Therefore, OrthoMTA would be readily dissolved by acid.
This study assessed cell cytotoxicity of test solutions to murine macrophages with WST-8 assay. WST-8 is highly water-soluble tetrazolium salt. It is reduced by dehydrogenase activities in cells to give a yellow-color formazan dye, which is soluble in the tissue culture media. Cytotoxicity of test solutions was assessed for macrophages because they appear in the inflamed periapical tissues.35 Macrophage is involved in cell-mediated innate immunity which phagocytoses opsonized microorganisms and dead cells. EDTA exhibited more cytotoxicity than CA or GA. This result is in accordance with a previous study where more toxicity of 17% EDTA was identified on murine macrophage than 15% CA in periods from 1 to 7 days.36 The elevated cytotoxicity of EDTA might be related to the chelation itself, and also to the accentuated decrease in pH.36 Segura et al.37 reported that EDTA reduced vasointestinal peptide binding to macrophage membranes that are responsible for the modulation of periapical immune response. If macrophage functions were altered, the phagocyte activity of inflammatory cells will not occur. Consequently, periapical healing will be inhibited. Further cytotoxicity experiments should be performed on periodontal ligament cells.
GA is an organic acid, commonly used in the beauty and cosmetic industry for peeling skin. Concentrations under 10% are considered mild and are used extensively in the beauty industry.38 It has little to no odor and it is not flammable. The lowest concentration of GA that could dissolve OrthoMTA in a minute was 5% in the pilot study. When GA was diluted to 2.5%, it took at least five minutes to weaken the surface of set OrthoMTA. And 1% GA merely weakened the surface of OrthoMTA in five minutes. So we made 5% solution by dilution of 70% GA (Junsei chemical, Tokyo, Japan) with distilled water. Its cell viability was superior to 17% EDTA in this study with less erosion to dentin. Therefore, it can be used in root canal treatment to dissolve OrthoMTA. Meanwhile, it is recommended to use organic acid in root canal treatment as short time as possible in order to prevent severe decalcification and weakening of teeth. Application of ultrasonic tip would promote retrieval of OrthoMTA.11 Further studies are needed to assess usefulness of ultrasonic tip in removal of MTA with 10% CA or 5% GA.
In this study, 10% CA and 5% GA reduced microhardness of set OrthoMTA in five minutes. Push-out bond strength test or direct removal of OrthoMTA from the root canals should be performed to determine usefulness of the solutions in retrieval of OrthoMTA.
Conclusions
Under the limitation of the present study, tested acidic solutions reduced microhardness of root dentin. Five minute's application of 10% CA and 5% GA showed significantly lower surface microhardness of set OrthoMTA with higher microhardness value of dentin and lower cellular cytotoxicity than 17% EDTA. 10% CA and 5% GA can be used as OrthoMTA dissolving solutions.




 XML Download
XML Download