

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Nickel-titanium (NiTi) engine-driven instruments are widely used for canal preparation. However, their fracture associated with flexural and torsional stresses is a notable disadvantage.1 When used according to specific guidelines, these instruments perform well.2 The procedure usually involving three steps (NGP), initial canal negotiation (N), glide path creation (G) and canal preparation (P), allows the clinician to successfully prepare most root canals with NiTi engine-driven instruments.2
In some instances, with a complex anatomy such as an abrupt apical curvature, canal negotiation should be performed with small pre-curved stainless steel (SS) hand files used in reciprocating motion, a watch winding motion.2,3 This procedure can be difficult, time consuming and challenging.3 Moreover, the conventional use of NiTi engine-driven instruments should be avoided in these instances for glide path creation and canal preparation.2,3 Instead, pre-curved SS and pre-curved NiTi hand files should be used, also with a watch winding motion. This procedure can be demanding and frustrating and could result in an increased incidence of procedural errors regardless of the clinician's expertise.3,4
The purpose of this article was to introduce a novel technique that allows safe and predictable NGP with reciprocating engine-driven instruments in canals where the use of conventional rotary files is contraindicated. This technique also eliminates the need for initial canal negotiation with small pre-curved hand files.
Case Report
The described technique is simple and straightforward. It involves the use of an Mtwo size 10 and 4% tapered instrument (Mtwo 10.04, VDW Dentsply, Munich, Germany) for canal negotiation and preparation of a glide path, and a Reciproc R25 instrument (R25, VDW Dentsply) for canal preparation. Both instruments are used in a forward (FW) and reverse (RV) direction in conjunction with a contra-angle connected to a motor that allows the reciprocating movement. The FW and the RV rotations are set on the motor at 6 degrees and 1 degree, respectively. The rotational speed is set between 25 - 50 rpm. All procedures are accomplished with the continuous intracanal use of a lubricant and/or a 2.5% solution of sodium hypochlorite.
The working length is estimated from an adequately exposed pre-operative radiograph. The canal negotiation and glide path preparation procedures are performed simultaneously with a straight Mtwo 10.04 using a slow pecking motion and without apical pressure. The amplitude of the pecking motion is approximately 3 - 4 mm. After 3 - 4 pecks, the Mtwo 10.04 is pulled out of the canal, cleaned with gauze, and reinserted and employed in the same manner. This step is repeated until the instrument reaches the working length. The progression of the instrument in the canal is monitored with the aid of an apex locator. Once the Mtwo 10.04 has reached the working length which is confirmed radiographically, the preparation is continued, in a similar manner, and completed with a straight R25.
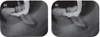
During the initial canal negotiation and preparation of a glide path with the Mtwo 10.04, the instrument may stop from advancing, an indication to the possible presence of a complex canal anatomy such as an abrupt apical curvature or ledge. The Mtwo 10.04 is pulled out of the canal and cleaned with gauze. Its tip is pre-curved (Figure 1) to allow the instrument to successfully negotiate and bypass the canal impediment. The instrument is reinserted and employed in the same manner until the working length is reached (Video 1). The working length is verified radiographically and the preparation is resumed with a straight R25 to the desired length. Similar to the Mtwo 10.04, the tip of the R25 should be pre-curved (Figure 1, Video 2) if the instrument stops from advancing in the canal (Figure 2). The tip of the instruments must be checked repeatedly to be certain that the curve is maintained. Any additional enlargement can be completed with the R40 or R50 reciprocating instruments (VDW Dentsply) with similar motor settings (Figure 2a), or with pre-curved NiTi hand files depending on the complexity of the canal anatomy and/or the abruptness of the canal curvature.
Discussion
Conventional canal negotiation with small hand files, a prerequisite prior to using an engine-driven instrument, is a delicate phase in canals with a complex anatomy.2,3 Iatrogenic errors could occur regardless of the clinician's proficiency.3 A straight size 10 file may not be able to reach the working length in approximately 7% of canals due to the presence of a complex anatomy such as an apical abrupt curvature despite the presence of apical patency.5 In these canals, the clinician uses pre-curved hand files size 8 and 10 with a watch winding movement and very small axial in and out movements in order to find the canal path and establish patency.3 This procedure can be demanding and frustrating because the amplitude of the left and right rotations associated with the watch winding movement may be too large to enable the clinician to find the canal path.3 The clinician faces this challenge every time the file is pulled out of the canal and re-inserted in order to locate the canal path, to confirm an open pathway and to reach the working length.3 Every attempt to negotiate those canals with small hand files could result in canal blockages and aberrations.3,5 There is also an increased risk of instrument fracture. The clinician cannot control the amount of torque applied on the hand instruments during the watch winding movement.3 The torque levels can easily exceed the elastic limit of these small instruments used in narrow and curved canals resulting in deformation of the instruments and their fracture. Moreover, the use of small NiTi rotary files for initial canal negotiation has been associated with a high incidence of instrument deformation and fracture.6
In similar situations with a complex anatomy, glide path enlargement should be provided with pre-curved SS or NiTi hand instruments used in reciprocation, watch winding.3 The clinician will then face challenges similar to those encountered during the use of hand files for the canal negotiation, including procedural errors and instrument fracture regardless of the clinician's proficiency.3,4
The M4 handpiece (SybronEndo, Orange, CA, USA) oscillates 30 degrees in both FW and RV directions. It can be used with small SS hand files for initial canal negotiation and glide path management.7 However, using the M4 handpiece in canals with a complex anatomy such as an abrupt curvature can also be challenging because the canal negotiation and glide path preparation are first accomplished by hand with pre-curved SS files up to size 15, then the M4 handpiece is secured to each file while still in the canal. The other concern associated with the M4 handpiece is the use of larger angles of reciprocation, compared to the described technique, leading to significant fatigue and torsional stresses especially in canals with a complex anatomy.8,9,10 Moreover, larger angles of reciprocation would result in more canal transportation and less centered preparations.10
Unless a glide path can be confirmed with a straight size 15 or 20 hand file, the canal preparation should be accomplished with pre-curved hand files.2,3 In addition to the challenge associated with this procedure, the risk of iatrogenic mishaps including instrument fracture is a concern especially in the presence of apical impediments.3
Considering the aforementioned risks associated with the conventional N.G.P. management of canals with a complex anatomy, the introduction of a technique allowing a reproducible, safe and effective mechanical N.G.P. would be beneficial. The technique described involves the use of NiTi engine-driven instruments (Mtwo 10.04 and R25) in reciprocation for canal negotiation, creation of a glide path and canal preparation. The Mtwo 10.04 has been frequently used for glide path management in continuous rotation.6,11 Its size at the tip (0.10 mm) and its 4% taper would allow effective canal negotiation and adequate glide path preparation in curved canals. The Reciproc R25 instrument has already been used in reciprocation for canal preparation.5 It has a 0.25 mm diameter at the tip and an 8% taper over 3 mm from its tip.
A straight size 10 hand file could not reach the working length in approximately 7% of the canals in mandibular molars despite the fact that canals were radiographically visible to the entire length.5 In addition, at least one study observed initial apical sizes 20 and higher in mandibular molars.12 These findings implied that the canal size was not an obstacle to the advancement of the hand file and that a complex anatomy, an abrupt curvature for instance, prevented the size 10 hand file reaching the working length during the initial canal negotiation. The author's impression was that a size 10.04 instrument should be able to reach the working length if the complex anatomy was adequately managed.
In the described technique, the simultaneous use of reciprocation and pecking motion reproduced the movement imparted to hand files during the conventional NGP procedure. The small degrees of FW and RV rotations were selected for 3 reasons. First, they would allow predictable finding of the canal path. Second, smaller angles produced better centered preparations and less canal transportation.10 Third, smaller angles reduced fatigue and torsional stresses which would compensate for the shorter fatigue life associated with abrupt canal curvatures (Figures 2 and 3).8,9,10 One study demonstrated that fatigue could be eliminated with very small degrees of rotation under severe stress conditions.9
The small angles of rotation recommended for the described technique were based on the endurance limit (EL) concept. The EL of a material is by definition the level of stress or strain (i.e. angle of rotation) at which a material can be subjected to 106 cycles without failure, a cycle corresponds to loading stress or strain, and releasing.9,13 Pre-curving an instrument results in its weakening due to the development of internal stresses. At the EL, continued cycling of the instrument is unrestricted, would not decrease the strength of the instrument any further and would not lead to the failure of the instrument. Very small angles of rotation, close to the EL angle of an instrument at which the fatigue life is unlimited, would allow using a pre-curved engine-driven instrument in reciprocation for NGP without the risk of fatigue-induced instrument fracture regardless of the abruptness of the canal curvature or its severity.9 Additionally, the risk of fracture from taper lock is eliminated considering that the angles of rotation set on the motor would be well below the elastic limit angle and the fracture angle of the instrument. Instrument fracture associated with fatigue and torsional stresses could be eliminated. Considering the benefits of reciprocation at small angles, engine-driven SS instruments could be used safely and efficiently for initial canal negotiation, glide path preparation and canal preparation even in the 2nd mesio-buccal canals in maxillary molars (Figure 4, Video 3).14 The use of SS instruments in reciprocation would offer a significant cost advantage to dentists in emerging countries.
A modification in the described technique consists in preparing the canal with a straight R25 as previously described without initial negotiation and glide path preparation.15 The FW and RV angles of rotation are set at 6 degrees and 1 degree, respectively. The progression of the R25 is controlled electronically with an apex locator until it reaches the desired working length. The use of the R25 without prior canal negotiation and glide path management can be accomplished safely and efficiently in the majority of the canals.5 If the instrument encounters resistance to progression or if it stops from advancing, canal negotiation and glide path preparation can be accomplished with a pre-curved Mtwo 10.04 instrument used as described. The preparation of the canal is then completed with the R25 to the working length; similarly to the Mtwo 10.04, the R25 can be pre-curved if it stops from advancing.
Ledge formation observed during canal preparation is a common complication which might adversely affect the outcome of the endodontic treatment. Locating and negotiating the original canal path can be difficult. Patience, perseverance and skill are essential requirements for bypassing ledges.16 The use of small pre-curved hand files with small left and right rotations and a pecking motion has been described to attempt bypassing a ledge. The clinician should aim to redirect the tip of the file to coincide with the original path of the canal.16 Similar to in canals with an abrupt apical curvature, a rotary file should not be used to attempt bypassing a ledge unless an adequate glide path is prepared with at least a size 15 hand file. However, the use of hand files for this purpose could result in additional endodontic mishaps regardless of the clinician's skills.3,4 The present technique combining the use of very small FW and RV rotations, pecking motion and a small pre-curved engine-driven NiTi instrument would allow the successful management of N.G.P. in the presence of a canal ledge.
Some canals may present calcifications or blockages which would prevent the advancement of files in the canal despite perseverance and numerous attempts. Such canals could be safely managed with this new concept of N.G.P. and the use of very small angles of rotation due to the elimination of instrument fracture, resulting from taper lock and fatigue. Apical pressure could be safely applied on the instruments to obtain patency if required (Figure 5). However, caution is required in curved canals to avoid canal transportation if patency is not achieved quickly.
The motor used to for the canal preparation was a prototype. The endurance limit of the R25 instrument was determined at 6 degrees (unpublished results). This angle was used for the FW, cutting direction. The reverse angle of rotation was determined by trial and error and set at 1 degree to obtain a faster reciprocation movement compared to higher angles. A higher RV angle of rotation would mean a longer time in this direction and, therefore, a slower reciprocating (FW and RV) movement. The speed, set between 25 - 50 rpm, was also determined by trial and error and was chosen because it allowed, in combination with the specific angles, an adequate cutting efficiency without a screwing-in effect.
Conclusions
A novel technique for canal negotiation, glide path preparation and canal preparation with NiTi engine-driven instruments used in a FW and RV movement is described. This technique eliminates the use of small hand files for canal negotiation. It also allows achieving predictable results in canal negotiation and glide path preparation not otherwise possible. The small FW and RV angles selected would allow a canal preparation technique without the risk of instrument fracture. The preliminary experience with this technique and the first impression were encouraging. However, the need for proper laboratory and clinical evaluation is warranted.




 XML Download
XML Download