

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The goal of apical periodontitis treatment has been to eliminate or substantially reduce microbial infection and to prevent re-infection by creating a tight seal of the root canal system.1,2 Bacteria involved in persistent infections may sometimes colonize the dentinal tubules of the main canal or the apical third of the canal near the apical foramen.3,4,5 In these areas, root canal instrumentation, including canal enlargement and shaping, could improve the canal disinfection. Nevertheless, in most clinical failures in which the root canals were properly managed, the bacteria are still present in the root canal system including in the dentinal tubules, isthmi, lateral canals, and apical ramifications.3,4,5,6,7,8,9
Lateral canals and apical ramifications of the main root canal are formed after a localized fragmentation of the epithelial root sheath develops, leaving a small gap, or when blood vessels that run from the dental sac through the dental papilla persist.10,11 Lateral canals are located in the coronal or middle third of the root, and usually extend horizontally from the main canal. Apical ramifications refer to the branching of the main canal into multiple accessory canals at or near the apex.3 A study reported that 70% of the root apex of teeth with refractory apical periodontitis that did not respond to root canal treatment had significant apical ramifications within their root canal systems.12 With maxillary central incisors, the incidences of anatomical complexity including lateral canals and apical ramifications have been reported in a wide range from 24 to 60%.3,5 Although there has been continuous debate about the correlation between harbored bacteria in the root canal system and the outcome of root canal treatment, it is obvious that open and large lateral canals could create a two-way passage of bacteria and tissue degradation products between the root canal space and periodontal tissue.13,14,15,16
This case report presents surgical endodontic management outcomes of maxillary incisors which were infected via the lateral canals.
Case Reports
Case 1
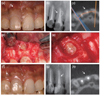
A 28 year-old man reported to the Department of Conservative Dentistry at Kyung Hee University Dental Hospital at Gangdong with the chief complaint of sinus tract that was adjacent to tooth #11 (Figure 1a). Due to the extensive caries, the patient had received an endodontic treatment and resin restoration 10 years ago. The patient did not report any spontaneous pain, and the tooth was asymptomatic to percussion and palpation. The sinus tract was traced with a gutta percha cone, which indicated that it was not toward the apical third but toward the middle third of tooth #11 (Figure 1b). A crack or anatomic variation was suspected and cone-beam computed tomography (CBCT, i-CAT, Imaging Sciences Internaional Inc., Hafield, PA, USA) was performed as a complementary examination. The CBCT image showed pararadicular radiolucency which was located in the middle root surface of tooth #11, and a crack or vertical root fracture was not observed (Figure 1c). Based on the clinical and radiographic findings, the tooth was diagnosed with a chronic apical abscess and surgical endodontic treatment was planned.
Under local anesthesia, mucoperiosteal flaps were raised. Upon elevation of the flap, vertical root fracture was observed along the root surface of the tooth #11 (Figure 1d). Examination of the root surface under the microscope confirmed that the lateral canal was the origin of the persistent periradicular lesion. The granulation tissue was removed and the lateral canal which was located in the middle one third of root was prepared using an ultrasonic tip (KiS-1D, Obtura Spartan, Fenton, MO, USA). The prepared lateral canal was filled with IRM (Dentsply DeTrey GmbH, Konstanz, Germany) and the flap was sutured with 4-0 blue nylon (AILEE CO., Busan, Korea) (Figure 1e). Additional curretage was not performed in periapical area.
The sutures were removed 1 week later, and the patient did not report any postoperative pain or discomfort. At the 1 month follow-up visit, the labial sinus tract was resolved (Figure 1f) and coronal re-restoration was performed. Twelve months after the procedure, periapical radiograph revealed healthy periradicular tissues (Figure 1g). The CBCT was taken 18 months after treatment and formation of the alveolar bone in the labial surface of tooth #8 was observed (Figure 1h).
Case 2
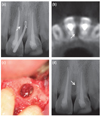
A 23 year-old man presented to the Department of Conservative Dentistry at Kyung Hee University Dental Hospital at Gangdong for treatment of a draining sinus tract, which the clinician found to be associated with tooth #21. The tooth had received endodontic treatment several years ago. Clinical examination revealed a sinus tract in the labial attached gingiva adjacent to tooth #21, as well as tenderness to palpation in the mesial periapical region (Figure 2a). Radiographic examination revealed alveolar bone resorption on the mesial surface of the root. There was no periapical lesion but gutta percha traced the lateral lesion of tooth #21 (Figure 2a). A CBCT image confirmed the mid-root mesial bone loss in tooth #21 (Figure 2b). Based on the clinical and radiographic findings, chronic apical abscess was diagnosed and surgical endodontic treatment of a tooth #21 was planned.
Under local anesthesia, mucoperiosteal flaps were raised in the area of tooth #21. An osseous defect over the mesial surface of the root was observed. The defect was degranulated, exposing the mesial root surface. Under a microscope, a large lateral canal in the cervical one third of the root was detected. A lateral canal was retro-prepared with an ultrasonic tip (KiS-1D) and sealed with IRM (Figure 2c).
One month after the surgery, the patient did not present with a sinus tract. At the six month follow-up visit, there were no clinical or radiographic signs of apical surgery failure (Figure 2d).
Discussion
Nonsurgical endodontic treatment is a predictable and reliable treatment with high success rates that range from 86 to 98%.15,16 Nevertheless, there are some cases in which the treatment has followed the highest technical standards and yet the treatments are unsuccessful.17 Some factors may be associated with the unsatisfactory outcome of well-treated cases. Song et al. examined the clinical causes of failure and the limitation of a previous endodontic treatment by examining the root apex and resected root surface at x26 magnification during the endodontic microsurgery of failed teeth that had undergone a previous endodontic treatment.18 The most common possible cause of failure was perceived leakage around the canal filling material (30.4%), followed by a missing canal (19.7%), underfilling (14.2%), anatomical complexity (8.7%), and other factors (8.8%). In the large majority of teeth with apical periodontitis, microbial infection was present not only in the main root canal but also propagated to anatomical complexities including dentinal tubules, recesses, isthmi, lateral canals, furcal canals, and apical ramifications.19 In this present case report, bacteria that persisted after treatment were arranged in biofilm structures located in an intricate network of the lateral canal that remained apparently unaffected by treatment.
Previously treated teeth with persistent periapical lesion(s) might be preserved with nonsurgical retreatment or endodontic surgery. However, it appears that the recommendations are often subjective and inconsistent, and there is a lack of consensus among dental professionals when making decisions related to retreatment or endodontic surgery.20,21,22,23 Torabinejad et al. reported that endodontic surgery offers more favorable initial success, but nonsurgical retreatment offers a more favorable long-term outcome.24 In first case, incomplete root canal filling and coronal restoration was observed. Therefore, the best treatment plan should have been nonsurgical endodontic re-treatment prior endodontic surgery.
Lateral canals, with few exceptions, are not visible in preoperative radiographs.10,25 The occurrence of lateral canals are usually suspected only when there is a localized thickening of the periodontal ligament on the lateral surface of the root or when a lateral periodontitis lesion is present.10 After root canal obturation, lateral canals can also be visualized on radiographs when a consistent amount of filling material is forced into the ramifications by compaction.6
Currently, there is debate among clinicians about how lateral canals should be filled. Previous studies investigated root filled teeth in humans and reported no relationship between unfilled lateral canals and the inflammation at the periradicular tissues.8,26 However, lateral canals and apical ramifications have been implicated in endodontic treatment failure when they are sufficiently large enough to harbor significant numbers of bacteria and to provide these bacteria with access to the periradicular tissues.10 The infection could be related to the size and patency of the lateral canals and apical ramifications as well as the microbiological conditions.11 A morphological study of 100 permanent molars revealed that 79% had lateral/accessory foramina with diameters that ranged from 10 - 200 mm.11 The largest diameter of lateral/accessory foramina was nearly two to three times smaller than the mean diameters reported for the main apical foramen.27,28 These differences in diameters between the main apical foramen and lateral/accessory foramina could explain why apical periodontitis is observed far more than lateral periodontitis.
Vieira et al. reported that a persistent intraradicular infection can be caused by bacteria located within dentinal tubules.29 Even though the lateral canal may appear to be "filled" on radiography, the histologic findings revealed that the filling material was intermixed with necrotic tissue and adequate filling of the lateral canal did not occur. Despite the radiographic normal periradicular conditions, histologic sections demonstrated that the lateral canal was actually not filled and that there were varying degrees of inflammation in residual tissue islands.10
Kim and Kratchman suggested that at least 3 mm of the root-end must be removed in root-end resection because 98% of the apical ramifications and 93% of the lateral canals exist in 3 mm of the root-end.30 The incidence of accessory canals located in the apical 3 mm was reported as 46%, 29% and 38% for the maxillary central incisors, lateral incisors and canines, respectively.7 The accessory canals in the maxillary central incisor were observed mainly on the labial side of the root. These could still be treated with surgical endodontic treatment even if they remain after the 3 mm resection. In this present case report, the infected lateral canals of the maxillary central incisors were located in the middle or cervical one third of the root and those were labially presented so that infected lateral canals could be successfully managed by surgical endodontic treatment without the root end resection.
Conclusions
This case report highlights the clinical significance and management of maxillary incisor lateral canals. It is important to be aware of root canal anatomic variability such as lateral canals and apical ramifications to determine proper surgical root canal treatment. Based on follow-up observations presented in this study, maxillary incisors infected via lateral canals can be successfully managed by surgical endodontic treatment.
 XML Download
XML Download