

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
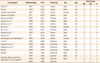
The anatomy of the tooth has long been an unresolved mystery. Successful root canal therapy depends upon identification and negotiation of all the canals, their subsequent cleaning and shaping and finally three-dimensional obturation of the entire root canal system. A major reason for endodontic failure is when extra roots or root canals are present are not detected.1 Traditionally, the maxillary first molars are generally described to have 3 roots, 1 palatal and 2 buccal, with each root having 1 canal. There is a wide range of variation in the literature with respect to the frequency and the number of canals in each root. The mesiobuccal root of the maxillary first molar contains a double root canal system more often than a single canal, and the incidence of second mesiobuccal canal (MB2) has been reported to be between 18.6% and 96.1%.23 The incidence of second distobuccal canal (DB2) has been reported to be between 1.6% and 9.5%.45 The incidence of two root canals in the palatal root has been found to be 0.2% to 7.0%.24 Apart from these anatomical aberrations, in extremely rare cases, the presence of a third canal in the mesiobuccal (MB3), distobuccal (DB3) and palatal roots has been reported.6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23 Case reports of maxillary first molars presenting with 3 or more root canals in a single root are summarized in Table 1.
This case report describes the diagnosis and successful endodontic management of a three-rooted maxillary first molar presenting with seven root canals: three canals each in the mesiobuccal and distobuccal root and one in the palatal root.
Case Report
A 26 year old male patient reported to the Department of Conservative Dentistry and Endodontics with a chief complaint of pain in upper right posterior region of mouth for the past one week. The patient revealed a history of mild intermittent pain for the past 2 months, which had increased in intensity during the past one week. The patient reported subjective symptoms of prolonged sensitivity to hot and cold food and drinks. The pain was spontaneous and aggravated particularly at night, and the patient required to consume analgesic to get relief from pain. The general anamnesis contained no abnormal data. Clinical examination revealed a deep disto-occlusal and mesio-occlusal carious lesions on the right maxillary first (tooth 16) and second molar (tooth 17) respectively. Palpation of the buccal and palatal aspects of the involved teeth did not reveal any tenderness. However, the tooth 16 was tender to vertical percussion, whereas tooth 17 did not reveal any tenderness. The teeth were not mobile and periodontal probing around the teeth was within the physiological limits. Thermal testing of the involved tooth with heated gutta-percha (Dentsply Maillefer, Ballaigues, Switzerland) and cold spray (Roeko Endo-Frost spray, Coltene-Whaledent, Langenau, Germany) caused an intense lingering pain, whereas electronic pulp stimulation (Parkell Electronics Division, Farmingdale, NY, USA) showed pulpal vitality on both teeth. The preoperative radiograph revealed the carious lesions closely approximating the pulp with a widened periodontal ligament adjacent to the mesiobuccal root with respect to tooth 16 and no signs of periapical changes with respect to tooth 17 (Figure 1a). Based on sensitivity tests and radiographic findings, a diagnosis of symptomatic irreversible pulpitis with symptomatic apical periodontitis with respect to tooth 16 and symptomatic irreversible pulpitis with respect to tooth 17 were made and endodontic treatment was initiated.
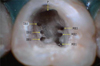
Radiographic evaluation of the involved teeth revealed three completely formed roots with no indication of any variation in the root canal anatomy (Figure 1a). The teeth were anesthetized using 1.8 mL 2% lidocaine with 1:200,000 epinephrine (Xylocaine, AstraZeneca Pharma Ind Ltd, Bangalore, India). The proximal surfaces of both the teeth were restored with composite resin (P60, 3M ESPE Dental Products, St Paul, MN, USA) after caries excavation to enable optimal isolation. Following rubber dam isolation, an endodontic access cavity was prepared on tooth 16 and 17. On inspection with a DG-16 endodontic explorer (Hu-Friedy, Chicago, IL, USA) under an operating microscope (Roslane Meditech, Haryana, India), the pulp chamber floor revealed two canal openings in the mesiobuccal root (MB1 and MB2), and one in the distobuccal (DB1) and palatal root on teeth 16 and 17. Anticipating the presence of extra canals, further exploration of the pulpal floor was carried out with a DG-16 endodontic explorer (Hu-Friedy) on tooth 16 on the line connecting the orifices of the buccal and palatal canal along the floor-wall junction. A "catch" just palatal to the orifice of the MB2 canal unveiled the third canal (MB3) in the mesiobuccal root. In addition, two sticky points were also detected on the line connecting the distobuccal and palatal canal orifices which led to the finding of two additional canals in the distobuccal root (DB2 and DB3, Figure 2). Inspection of the pulpal floor on tooth 17 was done for search of other orifices that were absent.
Even though initial visualization revealed additional canals present, however, several attempts to introduce a file into these orifices were unsuccessful. On further removal of dentinal shelf beginning from the orifice of the mesiobuccal and distobuccal canals and moving toward the orifice of the palatal canal with an ultrasonic micro-endodontic tip (ET 18D tip, Satelec Acteon, Merignac, France) clearly unveiled the orifice of additional canals. Negotiations of the canals were carried out with ISO size 06, 08, and 10 C-Pilot file (VDW GmbH, Munich, Germany) with clockwise and counter-clockwise rotational movement with apical pressure until the apex locator (Raypex5, VDW GmbH) reported that the apical patency was achieved. A glide path was established using size 15/0.01, 15/0.02 and 20/0.02 Hyflex Glide Path Files (Coltene-Whaledent) respectively. Coronal flaring was carried out using a NiTi size 25/0.08 Hyflex CM rotary instrument (Coltene-Whaledent) to improve the straight-line access. The working length which was initially determined with the help of an apex locator was later confirmed using individual radiographs for the mesiobuccal (Figure 1b), distobuccal (Figure 1c), and palatal root (Figure 1d) taken at different horizontal angulations. The working length radiographs showed that in the mesiobuccal root the MB2 canal merged with the MB3 canal at the apical third and exited through one apical foramen, whereas the MB1 canal had a separate canal orifice and exiting foramen. In the distobuccal root, the DB2 and DB3 canals merged with the DB1 canal at the middle and apical third respectively to form a single canal that exited through one foramen. Following which, the access cavities of both the teeth were temporized with a sterile cotton pellet and Cavit G (3M ESPE).
To confirm this rare and unusual morphology, dental imaging of the tooth with the help of CBCT (Carestream CS 9300, Carestream Dental LLC, Atlanta, GA, USA) was planned. An informed consent was obtained from the patient, and multi-slice scans of the maxilla was performed with a tube voltage of 90 KV and a tube current of 15 mA. All measures were taken to protect the patient from radiation. The involved tooth was focused, and the cross-sectional images were obtained in axial, transverse and sagittal planes (Figures 3a - 3e). All images were analyzed with the help of CS 3D imaging software (Carestream Dental LLC). Axial images were obtained at 180 µm thickness and were studied at cervical, middle and apical third of the roots to determine the canal morphology (Figures 3a - 3c). The images revealed that the tooth 16 had three roots and seven root canals (three mesiobuccal, three distobuccal, and one palatal). Transverse section CBCT scanned images of the mesiobuccal and distobuccal root confirmed the canal configurations that were seen in the working length radiographs (Figures 3d and 3e). In contrast, the contralateral tooth appeared to have a normal root canal anatomy (Figures 3a - 3e).
At the second appointment, the patient was asymptomatic. The tooth was anesthetized followed by rubber dam isolation. Cleaning and shaping was done using Hyflex CM rotary instruments along with lubricant (Glyde File Prep, Dentsply Maillefer, Tulsa, OK, USA) using the crown-down technique. All the mesiobuccal and distobuccal canals were enlarged to size 25/0.04, whereas the palatal canal was enlarged to size 40/0.04. Irrigation was performed using 3% sodium hypochlorite solution (Cmident, New Delhi, India) and 17% EDTA solution (Prevest Denpro Ltd, Jammu, India). The canals were finally flushed with sterile saline. Master cones were selected by placing gutta-percha cones (Dentsply Maillefer) corresponding with the size and taper of the last file used to the working length and was confirmed radiographically (Figures 1e and 1f). The canals were dried with absorbent points (Dentsply Maillefer), and obturation was performed using cold lateral compaction of gutta-percha and AH Plus resin sealer (Dentsply Maillefer). The tooth was then restored with a posterior composite resin core (P60, 3M ESPE). Final radiographs were taken to establish the quality of the obturation (Figures 1g and 1h). Tooth 17 was simultaneously treated using the same protocol as done for tooth 16. The patient remained asymptomatic during the 2 months of follow-up period.
Discussion
Out of the various comprehensive maxillary first molars ex vivo studies in the dental literature, only Baratto Filho et al. reported a maxillary first molar with three roots and seven root canals.24 Of the 140 extracted maxillary first molars, only one tooth showed seven root canals in which 3 mesiobuccal canals, 3 distobuccal canals, and 1 palatal canal were identified. However, all roots showed one apical foramen each.24 Kottoor et al. were the first to report a case of endodontic management of a right maxillary first molar with three roots and seven root canals.12 The tooth presented with 3 canals in the mesiobuccal root, 2 in the distobuccal root and 2 in the palatal root. Both the palatal and distobuccal root had a Vertucci type II (2-1) canal pattern, while the mesiobuccal root showed a Sert and Bayirli type XV (3-2) canal configuration.15 Kottoor et al. later reported the endodontic management of a left maxillary first molar with three roots and eight root canals.12 The tooth presented with 3 canals each in the mesiobuccal and distobuccal roots, and 2 in the palatal root. Both the mesiobuccal and distobuccal roots contained a Sert and Bayirli type XV (3-2) canal configuration, whereas the palatal root showed a Vertucci type II (2-1) canal configuration.12 More recently, Kumar and Badole et al. reported a case of endodontic management of a left maxillary first molar with three roots and seven root canals.67 The tooth presented with 3 canals in the mesiobuccal root, 2 in the distobuccal root and 2 in the palatal root. In the case reported by Kumar, both the palatal and distobuccal roots showed a Vertucci type II (2-1) canal pattern, whereas the mesiobuccal root canal showed a Sert and Bayirli type XV (3-2) configuration.6 In the case reported by Badole et al., both the palatal and distobuccal root showed a Vertucci type IV (2) canal pattern while the mesiobuccal root showed a Vertucci type VIII (3) canal configuration.7 In the cases reported by Kumar and Badole et al., the contralateral tooth also exhibited an identical morphology.67 Martins reported a unique case of endodontic management of a right maxillary first molar with three roots and seven root canals.25 The tooth presented with 4 canals in the mesiobuccal root, 2 in the distobuccal root and 1 in the palatal root. The mesiobuccal root showed a Sert and Bayirli type XXI (4-1) canal configuration, whereas the distobuccal and the palatal roots showed Vertucci type II (2-1) and type I (1) configuration, respectively.25
A literature review of the case reports presenting 3 canals in the mesiobuccal root of the maxillary first molar revealed a common Sert and Bayirli type XV (3-2) canal configuration.6891012141516171820 An exception seen was in the cases reported by Ayranci et al. and Du et al. who found a Sert and Bayirli type XVIII (3-1) and type XVI (2-3) canal configuration respectively.1113 On the other hand, Badole et al. and Beatty reported a Vertucci type VIII (3-3) canal pattern in the mesiobuccal root presenting with 3 canals.719 Karthikeyan and Mahalaxmi reported a case of endodontic management of a right maxillary first molar with six canals, 3 of which were located in the distobuccal root.21 The distobuccal root presented a Gulabivala's supplemental type III (3-2) canal configuration.21 Maggiore et al. and Wong reported a Sert and Bayirli type XVIII (3-1) canal configuration in the palatal root presenting with 3 canals.2223 In the present case, after correlating and computing the clinical, radiographic and CBCT scan findings, the configurations of the canals in the mesiobuccal and distobuccal roots were perceived to be Al-Qudah and Awawdeh type (3-2) and type (3-2-1), respectively. Figure 4 illustrates Al-Qudah and Awawdeh supplemental canal configurations.26
In 2006, Cleghorn et al. did a comprehensive review of the root and root canal morphology of the maxillary first molar from the data obtained from various anatomical studies.27 The internal canal morphology of the mesiobuccal root in 8,399 teeth was assessed in 34 laboratory and clinical studies. In this large sample, the prevalence of one canal (MB) was 43.1%, and the incidence of two canals (MB1 and MB2) was 56.8%. The incidence of one apical foramen in the mesiobuccal root was 61.6%, while two separate apical foramina were present in 38.3%. The canal morphology of the distobuccal and palatal roots was assessed in 14 laboratory and clinical studies that included 2,576 teeth. In the distobuccal root, the prevalence of one canal (DB) was 98.3%, and the incidence of two canals (DB1 and DB2) was 1.7%. A single apical foramen was present 98% of the time. In the palatal root, the prevalence of a single canal and a single foramen were 99% and 98.8%, respectively. One common finding in this extensive review was the absence of any study reporting the presence of the third canal in any of the three roots.27
However, more recent anatomical studies were able to establish the prevalence of the third canal in the mesiobuccal root. Degerness et al. sectioned and examined 90 uninstrumented mesiobuccal roots of maxillary first molars under stereomicroscope, and found that MB3 has an incidence of 1.1%.28 Using CBCT, Lee et al. and Kim et al. analysed 458 and 814 maxillary first molars, respectively, and reported a prevalence of MB3 of 1.3% and 0.1%, respectively.2930 Verma et al. and Kim et al. documented an incidence of 10% and 12%, respectively.3132 The study from Verma et al. had a small sample of 20 roots, and the results may not have a very strong statistical value.31 However, the study from Kim et al. had a sample of 154 roots and must be considered as a frame of reference.32
The higher incidence of multiple canals in the mesiobuccal root as compared to the distobuccal root could possibly be due to the mesiobuccal root being broad buccolingually while the distobuccal root is round or ovoid in cross-section.27 Sometimes fusion of distobuccal root with palatal root may occur due to distobuccal root being broad buccolingually and may result in additional canals in the distal root. In the present case, axial and transverse section of CBCT scanned images clearly depicted that the mesiobuccal and distobuccal roots were broad buccolingually with distobuccal root fused with the palatal root (Figure 3b), confirming that this variation in the external root morphology may account for the multiple canals found in them.
Conclusions
This report serves to remind the dental practitioners of the complexities in root canal morphologies that the maxillary first molars can exhibit. A clinician should have a thorough knowledge of all the diversities and should perform careful examination of the floor of the pulp chamber with a dental operating microscope, and use advanced diagnostic aids such as CBCT for the success in endodontic treatment.



 XML Download
XML Download