

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Dental caries is one of the most prevalent chronic diseases affecting humanity. Its progression or control depends on the balance between pathological and protective factors, and the best strategy for caries management is focused on methods of improving the remineralizing process.12 When a restorative intervention is necessary, the use of materials with minimal aggression to the tooth structure and cariostatic, adhesive, and biocompatible properties must be prioritized.3 Since their introduction by Wilson and Kent and clinical development by McLean and Wilson, glass ionomer cements (GICs) have been largely used in restorative dentistry because of their ability to reduce the incidence of caries affecting unrestored tooth surfaces.4567891011 One of the main characteristics of GICs is their continuous fluoride release, allowing reduction of the mineral dental structure solubility and inhibition of microbial metabolism and favoring re-establishment of the balance of the oral environment.512131415
Fluoride ions are essential elements in the prevention and treatment of dental caries.315161718 Thus, many new studies are interested in finding ways to maintain fluoride ions in the oral environment, particularly at the interface of the tooth with a bacterial biofilm.1519 The measurement of fluoride ions released within a determined period of time is one of the applicable methodologies to evaluate the cariostatic properties of GICs for in vitro studies. This evaluation, associated with laboratory tests such as adhesive and physical resistance and manipulation characteristics, guides the choice of materials for clinical practice.20
Laboratory tests demonstrated that fluoride release varies in accordance with the cement category - conventional or resin modified - and a variation among cements in the same category can also be seen. This affirmation can be inferred from the different results obtained by several researchers for different tested materials.12131721222324252627 However, there is no consensus on the principal factor responsible for the variation of fluoride release from ionomer cements, that is, whether the difference is due to the cement category or the specific composition of some materials, independent of their category. Therefore, the present study aims to compare the fluoride release of five new and three established brands of conventional and resin-modified GICs. The null hypothesis of the study is that there is no difference between conventional and resin-modified GICs with respect to the fluoride release.
Material and Methods
The fluoride release from the GICs tested was analyzed in an experimentally designed in vitro study. The materials used are listed in Table 1.
Immersion media
Three different solutions were used during the fluoride release test. 1) Total ionic strength adjustment buffer II (TISAB II), a buffer solution containing deionized water, acetic acid, sodium chloride, and cyclohexane-diamino-tetra-acid (CDTA), which was used to provide constant background ion strength, decomplex F to make it available for determination, and adjust the solution pH. 2) Demineralization solution containing deionized water, calcium chloride dehydrate, sodium phosphate monobasic, acetate buffer, sodium hydroxide, and thymol and having a pH of 4.3, in which the specimens were immersed for 6 hours a day. 3) Remineralization solution containing deionized water, calcium chloride dehydrate, sodium phosphate monobasic, potassium chloride, tris(hydroxymethyl)aminomethane buffer (TRIS buffer), sodium hydroxide, and thymol and having a pH of 7.0, in which the specimens were immersed for 18 hours a day. Solutions 2 and 3 compose the pH cycling system used in this study. During the immersion period, the specimens were agitated using a shaker equipment at room temperature, and the storage solutions were changed daily as described above (after 6 hours in the demineralization solution, the specimens were immersed for 18 hours in the remineralizing solution).
Preparation of the specimens
Six disc specimens (8.60 mm in diameter; 1.65 mm in thickness) of each material were prepared using a standard stainless steel mold, two glass plates, and a transparent matrix in between. The tested materials were mixed in accordance with the manufacturer's recommendations at room temperature (25 ± 1℃). A piece of nylon thread was incorporated into the cement during setting to suspend the samples in the test medium. After 7 minutes, they were removed from the mold and placed in a humidifier recipient at 37℃, 100% humidity for 24 hours to simulate the oral environment.
Fluoride release measurement
The fluoride ion concentration was measured by the potentiometric method using a fluoride-specific electrode (Orion model 96-09, Orion Research, Cambridge, MA, USA) coupled with an ion analyzer (Orion SA-720, Orion Research) according to Carvalho and Cury (1999).23 The instrument was calibrated with a series of standard fluoride solutions (1.25 to 15.00 and 5.00 to 25.00 µgF/mL prepared in TISAB) according to the fluoride concentration of the samples. The specimens of each material were placed in plastic test tubes containing 2 mL of the remineralization or demineralization solution according to the pH cycling system, and after the immersion period, the same volume of TISAB was mixed for the fluoride analysis.
The fluoride release was measured for 15 days. To calculate the total daily fluoride release, the fluoride ion concentration found in the remineralization and demineralization solutions were added. The fluoride concentration was given in millivolts (mV) by the electrode and was converted into the quantity of fluoride per material area (µgF/cm2). Analysis of variance (ANOVA) and Tukey's test were used for the statistical analysis (α = 0.05).
Results
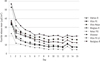
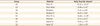
The daily mean fluoride release from GICs in the demineralization-remineralization (de-re) solutions over 15 days is displayed in Figure 1. Table 2 shows the cumulative fluoride release of each material over 15 days. The daily mean fluoride release during the test period for each material is presented in Table 3. The highest amount of fluoride was released by Vitro Fil (DFL), a conventional GIC, differing statistically from all other tested materials (p < 0.05). There were no statistically significant differences among Resiglass (Biodinâmica), Bioglass R (Biodinâmica), and Vitro Fil LC (DFL), or between Vitremer (3M ESPE) and Vidrion R (SS WHITE) (p > 0.05). The least amount of fluoride was released by Ketac Fil (3M ESPE), differing statistically from all other tested cements (p < 0.05).
A pattern of fluoride release was observed in all tested materials. The highest mean values of fluoride release were found in the first 24 hours, decreasing abruptly on day 2 and reaching gradually decreasing levels on day 7.
Discussion
Several studies tested the in vitro fluoride release from conventional and resin-modified GICs.17252628293031 However, the use of different methodologies and materials leads to a considerable variation of research results. Some of the factors related to in vitro fluoride release from restorative materials are the fluoride concentration in the set materials, size and composition of the inorganic filler, powder-liquid ratio of two-phase systems, mixing procedure, curing time, inner-material porosity, surface treatment and amount of exposed area of the specimen, and the type, temperature, and pH of the immersion media used.61215 Depending on the powder composition, the material is capable of releasing different amounts of fluoride. Hattab and Amin found a strong positive correlation between the released fluoride and the fluoride concentration in the set materials.12 Further, it is common knowledge that the inorganic filler composition of ionomer cements, compomers, and composite resins interferes with fluoride release.2526 Fluoroaluminosilicate glass is the major component filler of GICs. As it is more soluble than the barium and strontium present in most compomers and composites, it is able to release more fluoride.32 Particle size also has a significant influence on fluoride release. Reducing the filler particle size can increase fluoride release because smaller particles have larger surface areas.126
Reduction of the inorganic filler size in compomers and GICs is a way for manufacturers to increase fluoride release.526 Another item related to the release and recharge on fluoride ions is the material's porosity. Xu and Burgess found that higher porosity allows deeper diffusion of the recharge agent into the sample and results in more fluoride storage and release.26 They also reported that materials with less resin content, such as glass ionomers and resin-modified glass ionomers, have higher porosity and exhibit higher fluoride recharge capabilities than compomers or composites.
Regarding immersion media, the most cited ones in fluoride release methodologies are deionized water, saliva, artificial saliva, saline solution, and pH cycling system (de-re solutions).6812232733 An analysis of these findings reveals that pH and ionic saturation from an immersion medium can influence the quantity of fluoride released. Indeed, for conventional and resin-modified GICs, the highest fluoride release is found in acidic and de-re solutions.1530
The increasing amount of fluoride in acidic media can be explained by the fact that a decrease in pH increases the dissolution of the material, leading to a higher fluoride level in the acidic immersion.15 In the case of neutral solutions, Hattab and Amin observed that GICs released significantly less fluoride in artificial saliva than in deionized water.12 Besides the pH, the type of acid found in immersion solutions has an important effect on cement degradation.33 McKenzie et al. observed that solutions containing carboxylic acids, capable of chelating calcium ions present in the cement and forming complexes of reasonable solubility in water (such as in orange and apple juices), have shown a greater degradation potential over ionomer cements than solutions containing phosphoric acid (such as Coca Cola), which although capable of chelating with calcium, form essentially insoluble complexes.33 It is also important to explain that the degradation of ionomer cements is directly related to fluoride release.30
Carvalho and Cury, evaluating the fluoride released from different dental materials in deionized water, artificial saliva, and de-re solutions, concluded that de-re solutions were a better immersion medium for the specimens because of the better cariogenic challenge simulation, which could not have been conducted in deionized water or artificial saliva, whereas other elements such as pH and proteins potentially influence dissolution and erosion, as reported by Shiozawa.623 In the present study, the de-re solutions were chosen to represent oral conditions.
The use of a surface coating agent (SCA) over GICs can be controversial. Although manufacturers recommended protecting the ionomer cement against degradation in its first setting phase, the use of SCA in in vitro studies interferes with microleakage and significantly reduces ionomer cement fluoride release.12 Thus, covering freshly set glass ionomers with varnish or resin significantly reduces the rate and amount of fluoride released in both deionized water and artificial saliva.12 Further, unlike the in vivo physiological abrasion caused by SCA due to chewing, occlusal grinding, and tooth brushing, there is no abrasion during in vitro tests and a thin layer of fluid resin remains over the material.12 In such cases, an SCA was not used as it could not be removed because the finishing and polishing of the specimen would decrease its surface area, modifying the amount of fluoride release.
Williams et al., while analyzing the influence of the surface area and the volume of specimens during in vitro fluoride release tests, concluded that the quantity of released ions is directly related to the surface area of the specimen and that the volume does not have any influence on the quantity of ions released.24 Thus, finishing and polishing could change the specimen dimensions, resulting in possible alterations to the surface area. Otherwise, the specimens' superficial smoothness was obtained by a transparent matrix, which is a good substitute for finishing and polishing.
In the present study, the highest or lowest amounts of fluoride release of the tested GICs could not be justified by the material category, that is, conventional or resin-modified GICs. While the cement that released the highest amount of fluoride was a conventional GIC (Vitro Fil, DFL), the one that released the least amount belonged to the conventional category as well (Ketac Fil, 3M ESPE). The different methodologies applied to the in vitro fluoride release research and the absence of published research about the five new materials tested in the present study make it even more difficult to compare these results to other in vitro fluoride release results. Carvalho and Cury, using a similar methodology, found the daily means of fluoride release for Vitremer (12.27 ± 1.16 µgF/cm2) and for Chelon Fil (8.35 ± 0.51 µgF/cm2), agreeing with the results found with Vitremer and Ketac Fil in the present study.23 Other researchers have demonstrated the greatest fluoride release from Vitremer compared with Ketac Fil, Ketac Molar, and Fuji IX, all conventional GICs with regular viscosity (Ketac Fil) or high viscosity (Ketac Molar and Fuji IX).25272834 The explanation for the higher fluoride release by resin-modified GICs is as follows: Acid-based reactions are slowed down by the resin component, which makes the ionic matrix less mature and capable of releasing more fluoride, if compared with a conventional material of the same age; larger pore size and porosity of resin-modified GICs; low solubility and high powder-liquid proportion of GICs with high viscosity.252834
However, when a great variety of conventional and resin-modified GICs were compared, the variation of the amount of fluoride release could not be attributed to the type of material or GIC category; this is in agreement with the results of the present study.2635 Xu and Burgess found a negative linear correlation between the compressive strength and fluoride release and that restorative materials with high fluoride release had lower mechanical properties.26 This may be in accordance with other studies that attribute the rates of fluoride release to the solubility and erosion of GICs.330 Additionally, Xu and Burgess found a considerably large discrepancy in the amount of fluoride release within the resin-modified GIC category, from 162 µgF/cm2 (Vitremer, 3M ESPE) to 375 µgF/cm2 (Photac Fil, 3M ESPE), cumulated in 21 days.26
The fluoride release of conventional and resin-modified GICs follows the same pattern. Most of the reviewed studies mentioned that the tested materials present a significantly higher release during the first 24 hours, declining from day 2 and tending to stabilize towards day 7.131729 This may be caused by the initial superficial rinsing effect, while the constant fluoride release during the following days occurs because of the fluoride's ability to diffuse through cement pores and fractures.32 An initial high release from glass ionomers over the first 24 hours is likely due to the burst of fluoride released from the glass particles when reacting with the polyalkenoate acid during the setting reaction.15 In the present study, the higher means were observed on day 1, decaying from day 2, and then tenuously diminishing the fluoride release towards day 7.
Fluoride-releasing restorative materials, particularly GICs, present antibacterial properties and can affect in vitro conditions of the microbial metabolism during caries process simulation. However, prospective clinical studies did not verify whether the secondary caries incidence can be significantly reduced by these materials. The cariogenicity and frequency of the patient's diet, presence of saliva, and bacteria-producing acid challenges are important clinical variables to be considered.536 Dijkman et al. showed that a monthly cumulative fluoride release of 200 - 300 mg/cm2 is sufficient to completely inhibit enamel demineralization in vivo.37 In the present study, for a 15 day period, the materials that showed a fluoride release of 200 µg/cm2 or more were Vitro Fil, Vitro Molar, and Bioglass R among the conventional GICs, and Vitro Fil LC and Resiglass among the resin-modified GICs.
Conclusions
This study showed a wide variation among the materials in terms of the cumulative amounts of fluoride ions released. This variation was not related to the type of material. Therefore, the amount of fluoride released could not be attributed to the category of GIC, that is, conventional and resin-modified GICs, and this confirms the null hypothesis of the present study.


 XML Download
XML Download