

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The relationship between pulpal and periodontal disease was first described by Simring and Goldberg in 1964.1 In many cases it is easy to establish diagnosis, but there are certain cases, where situation becomes more complex, especially when it combines with periodontal disease. It becomes essential to correct periodontal defect simultaneously in these cases to prevent recurrence, and to improve functional status of the tooth.2 Various treatment modalities have been proposed earlier for the treatment of endo-perio involvement including open flap debridement, root resection and retrograde filling, where healing is by scar.3 Since this is not ideal, newer approaches such as regenerative procedures like guided tissue regeneration (GTR), bone grafts and growth factors that aim to restore lost tissue have been introduced. Platelet rich fibrin (PRF) enriched with platelets and growth factors promotes periapical tissue regeneration and healing. This case report presents an attempt to evaluate the healing kinetics of the combination of PRF and alloplastic bone substitute (Bioactive glass) as opposed to using these materials alone.
Case Report
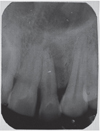
A 35 year old male patient reported to the Department of Periodontics with a complaint of pain in the upper left front tooth region associated with pus discharge for 2 months (Figure 1). He also gave history of trauma around 7 years back and noticed discoloration of tooth with time but he took no treatment as the tooth was asymptomatic. On intraoral examination there were no carious teeth. Intraoral periapical X-ray (IOPA) was taken which revealed radiolucency along the distal side of the entire root surface to the apex (Figure 2). Electric pulp testing was done to check the vitality of the tooth which confirmed that the tooth was non vital and the tooth was tender on percussion. Vertical probing depth was measured which was found to be 8 mm on distal side. Endodontic treatment was taken up first and then periodontal regenerative surgery was planned for treatment of defect.
On the day of surgery, PRF was prepared. Exactly 10 mL of whole blood was drawn by venipuncture of the antecubital vein and collected in two 5 mL sterile glass tubes coated with an anticoagulant, acid-citrate-dextrose. Whole blood was initially centrifuged (3,000 rpm for 10 minutes, Figure 3).The plasma was then aspirated with a micropipette and subjected to a second centrifugation at 2,000 rpm for 10 minutes, which allowed the precipitation of the platelets (0.8 to 1.2 mL) to fall onto the bottom. Coagulated preparation of 0.3 mL of PRF was obtained by its combination with 0.1 g of calcium chloride (Figure 4). Then graft material was mixed with the coagulated platelet rich plasma (PRP) preparation.
Surgical Procedure
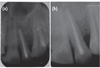
The area selected for surgery was anesthetized using xylocaine with adrenaline 1 : 200,000. A full thickness flap was raised at the labial aspect using intracrevicular incision (Figure 5). Thorough curettage of the defect area was done and a combination of PRF and bioactive glass was placed in the defect (Figures 6 and 7). Closure of soft tissue flap was done with non resorbable black silk (3-0) suture using interrupted suturing technique. The sutures were removed 10 days after surgery. The patient was scheduled for regular recall intervals at 3, 6, 9 and 12 months. PRF and bone graft resulted in substantial amount of bone fill (Figures 8a and 8b), and probing depth was reduced to 2 mm.
Discussion
Endo-perio lesions are common conditions that are difficult to diagnose. However, if patient's history is taken carefully and thorough clinical examination is done, these lesions can be treated completely to give favorable outcome. Data collected must include periapical radiographs, pulp vitality testing, cavity test, percussion, palpation, and pocket probing depth. In this report, history of trauma and the pulp vitality test which showed the nonvital nature of the tooth was a pivoting finding suggesting the endodontic involvement. Infrabony pocket of 8 mm on distal aspect of tooth indicated a secondary periodontal involvement requiring specific therapy to achieve success. The success rate of the endodontic-periodontal combined lesion without a concomitant regenerative procedure has been reported to a range from 27 to 37%.4 which suggests the need of surgical intervention. Recent advances in our understanding of cell regulation by growth factors present new options and provide additional treatment modalities for regenerating lost periodontal support.
The use of PRF is a recent and promising innovation in periodontal regenerative therapy. The positive impact of PRF on bone healing could be attributed to the angiogenic, proliferative and differentiating effects on osteoblasts of tissue growth factor β and platelet derived growth factor (TGF-β and PDGF) that are present in PRF in high concentrations.5 PRF has also been successfully used with different graft materials, with and without GTR, in the treatment of human periodontal infrabony defects.6-9 Bioactive glass enhances bone formation by ionic dissolution of ceramic material such that silica gel layer forms over the particles in contact with body fluids. Over the silica gel layer, a calcium phosphate layer forms which is quickly converted into hydroxycarbonate apatite layer.10 This apatite layer has been shown to identical with bone mineral and has provided surface for osteoblast cell attachment and bone dissolution.
PRP behaves like TGF-β to modulate cell proliferation in a specific manner which been shown to inhibit the epithelial cells while stimulating osteoblast and PDL cells.4 Fibrinogen converted to fibrin in combination with growth factors present in PRP may promote wound healing at the site of injury. As the blood clot stabilization is an important event in healing, PRF due to its high fibrin content may work as a hemostatic and stabilizing agent for the stability of the bone graft and blood clot.11 Attia has shown significantly favourable clinical improvement in periodontal infrabony defects with combination of PRF and tricalcium phosphate β (β-TCP) graft material.12
The healing potential of PRF combined with β-TCP has not been studied widely in endodontics. Kim et al. observed rapid bone formation, remodelling, and calcification in rabbits in the second week with combination of PRF with β-TCP than the β-TCP alone.13 In the present case, it was observed that at 3, 6, 9 and 12 months follow-up after the surgical treatment of large chronic periapical lesion, PRF combined with β-TCP resulted in significant clinical and radiographic bone regeneration.
Besides promoting wound healing, bone growth and maturation, PRF with bone graft have the advantages of graft stabilization, wound sealing, hemostasis and improved handling properties.14 However, like other case reports, this study also has limitations like short follow-up period of 12 months and a need for histological evaluation to confirm regeneration.
Conclusions
Endo-perio lesions are common conditions that are difficult to diagnose. However, if patient's history is taken carefully and thorough clinical examination is done, these lesions can be treated completely to give favorable outcome. The healing of an endodontic lesion is highly predictable, but the repair or regeneration of periodontal tissues is questionable if associated with it. Recent introduction of growth factors for periodontal treatment provide new opportunities for healing. This case report presents an attempt to evaluate the clinical effectiveness of the combination of PRF and β-TCP as opposed to using these materials alone. The use of autologous platelet preparations like PRF allows the clinician to optimize tissue remodelling, wound healing and angiogenesis by the local delivery of growth factors and proteins. The novel technique described enables the clinicians to gainfully harvest the full regenerative capacity of this autologous biologic material.






 XML Download
XML Download