

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Crown fracture is the most common type of traumatized anterior tooth.1,2 If the fractured fragment is available, reattachment of the tooth fragment can be the most favorable treatment option in terms of esthetic concerns.3 The reattachment of the fractured tooth fragment has advantages including the preservation of the remaining tooth structure, reproducibility of the tooth contour and natural colors, and the most well-preserved incisal transparency.4,5 For the reattachment of the fractured fragment, several options exist. Among these, the use of the glass-fiber post is a favorable option for the retention of the fractured segment.3 Zorba and Ozcan used a fiber-reinforced post to increase retention of the reattached crown fragment.6 However, the reattached fragment/post complex is susceptible to displacement if the retention is not sufficient. In this respect, the clinician can increase the retention of the complex by enhancing the fitness of the post for the prepared root canal. It was suggested that relining the post with composite resin can increase the retention of the fragment/post complex.7 However, no report has been published regarding the use of a relining technique using an indirect method on a working cast. Therefore, in this case report, we describe the indirect fiber-reinforced post relining technique with composite resin to increase fitness to the root canal and to reduce chair time. We also evaluate the esthetic concerns about dehydration of the reattached fragment.
Case Report
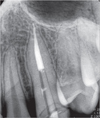
A 16 year-old male patient visited the clinic because of trauma, and an examination revealed a complicated crown fracture of the left maxillary canine (Figure 1). The fracture was caused by hitting a solid bowl, and the fractured surface had been separated neatly due to an instantaneously applied strong force. The labial margin was present 1 mm below the marginal gingiva, and the lingual margin was supragingival (Figure 2). The patient visited the clinic approximately 5 hours after the trauma, and the broken tooth was brought to the clinic in milk.
The comparison of the shape of the fractured fragment with the retained tooth structure indicated that there was no significant discrepancy. Additionally, the patient wanted to preserve the fractured fragment. Therefore, fractured fragment reattachment was performed after endodontic treatment, and a glass-fiber post was inserted into it for retention. Because the labial margin was located in the subgingival region, a gingivectomy was performed using an electro-surgery kit (PerFect TCS, Whaledent, Mahwah, NJ, USA) under 2% lidocaine HCl (Xylestesin-A, 3M ESPE, Seefeld, Germany) anesthesia. For post insertion, a post hole was prepared by extending half of the length of the root. When the suitability of the glass-fiber post (Luxapost, ø 1.5 mm, DMG, Hamburg, Germany) was examined, the width of the glass-fiber post was considerably smaller than the diameter of the post hole (Figure 3). Therefore, post relining was selected to improve fitness.
The indirect technique was considered to adjust the post relining and confirm the exact fracture line location. This technique was considered to be easy, to reduce chair time, and to make production easier. An impression was performed using Aquasil Rigid and XLV (Dentsply Caulk, Milford, DE, USA), and a working cast was fabricated with red stone. Relining of the glass-fiber post was performed using the method reported by Faria-e-Silva et al.7 Glycerin gel was applied to the working cast as a separating medium and air-thinned. The surface of the fiber post was treated with CoJet Sand (CoJet Sand, 3M ESPE), and a silane coupling agent (Calibra, Dentsply Caulk) was applied to it and then dried. A 1 : 1 mixture of a self-cure activator and adhesive (Prime & Bond NT, Dentsply Caulk) was applied to the surface of the post and light-cured for 20 seconds. After the post hole of the working cast was filled with composite resin (Filtek Z350, Body A3, 3M ESPE), the glass-fiber post was inserted into the hole to the length of the preparation and light-cured for 20 seconds (Figure 4). The relined post after removal from the cast was light-cured for an additional 20 seconds.
The inner surface of the fragment was minimally prepared, and the location where the post met the fractured fragment on the working cast was identified to perform an adhesion between the fractured fragment and the relined post. The inner surface of the fractured fragment was etched with 32% phosphoric acid (Phosphoric Acid Etchant, Bisco Inc., Schaumburg, IL, USA). A 1 : 1 mixture of a self-cure activator and adhesive (Prime & Bond NT) was applied to both the inner surface of the fractured fragment and the surface of the post and then, light-cured for 20 seconds. Calibra cement was mixed and applied to both the upper part of the post and the inner surface of the fractured fragment. After that, the relined post and the fractured fragment were positioned to make them fit to the fractured line on the working cast and then light-cured for 40 seconds (Figure 5).
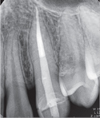
The root canal surface was etched with 32% phosphoric acid to perform reattachment of the fractured fragment intraorally. A 1 : 1 mixture of the self-cure activator and adhesive was applied to the root canal surface, the inner surface of the fractured fragment, and the relined post, and then, light-cured for 10 seconds. Calibra cement was applied to the root canal surface using a Lentulo spiral, and the relined post was positioned in the prepared post hole. This confirmed whether the transition state between the fractured fragment and the retained tooth structure was consistent. In addition, 10 seconds of light curing, excess cement removal, and then, 20 more seconds of light curing were performed.
After reattachment of the fractured fragment, the color of the fragment was a little brighter due to dehydration that was caused by the relatively long extra-oral time prior to intraoral delivery (Figure 6). There was also the damage in the marginal gingiva due to both chemical burns and irritation during adhesive luting.
Discussion
If the extra-oral time of the fractured fragment increases, dehydration of the fragment can occur. Therefore, in order to prevent this case, it is recommended that the fragment be kept in a medium such as physiologic saline.8,9 According to Toshihiro and Rintaro, even though the fractured fragment that was reattached was dehydrated, the fragment recovered its original color and translucency without any negative changes.10 In this case, the typical aesthetics of the tooth were recovered after a week. It is generally expected that fragment dehydration and discoloration will not have a significant impact on the final reattachment outcome.
Applying a post to accompany the fractured fragment for reattachment is associated with positive effects on prognosis due to increased retention of the fractured fragment and tooth structure reinforcement.11 In addition, in cases where the root canal diameter is very large, retention can be improved by increasing fitness to the root canal rather than increasing the length of the post.12,13 According to the research conducted by Faria-e-Silva et al. in 2009, the push-out strength values when post relining was performed were significantly higher than those when post relining was not performed in the apical, middle, and cervical 1/3 of root canals.7
Microleakage and subsequent detachment can occur over time, because the bonding interface increased with adhesion between the relined post and the fractured fragment during the reattachment that was performed in this case.14,15,16,17 Thus, accurate and careful bonding procedures are necessary through the course of treatment, and long-term tooth prognosis is also important to observe.
Conclusions
For post relining, the indirect technique is more advantageous than the direct technique that is applied intra-orally. The indirect technique can increase the composite resin curing rate and can determine whether the post is situated correctly in the prepared post hole, without the use of additional assessment tools.







 XML Download
XML Download