

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Although the etiological factors of dental caries and the methods for its prevention have been widely investigated, secondary caries is still the main cause for the replacement of restorations.1 Several investigations have revealed microgaps at the interface between dentin and adhesive restorations in vivo.2,3 This implies that even the latest adhesive systems are not capable of producing a complete seal in clinical situations. Once the gaps are formed, bacteria and their toxic products readily invade. The bacteria proliferate at the bonding interface, permeate the unsealed dentinal tubules, and may cause pulpal responses. Therefore, the possibility of adhesive systems having antibacterial effects is attractive with respect to the prevention of infections.
Elimination of bacteria during cavity preparation is another issue. Because it appears that only soft, wet dentin is heavily infected with bacteria, any techniques that effectively remove such infected dentin should be adequate to halt the carious process, if the cavity is then adequately sealed.4 In contrast, the removal of hard dry dentin, which is essentially only demineralized with relatively few bacteria present, would be unnecessary, and may result in the additional, unwarranted removal of a sound tooth structure and possible pulp exposure.5 Thus, after the removal of carious dentin, it is important to eliminate any remaining bacteria that may be present on the cavity walls, in the smear layer, at the dentinoenamel junction, or in the dentinal tubules.6 During the removal of carious tissue, bacteria invariably remain entrapped in the dentinal substrate because neither the clinical parameters of dentin hardness and color nor the caries-detector dyes are able to ensure the complete elimination of microorganisms.5,7 Bonding systems that have intrinsic antibacterial properties would be beneficial in this regard. As the contemporary dentin adhesive systems have not been proven to be completely effective in eliminating the microleakage at the tooth/restoration interface, the incorporation of antibacterial agents into the adhesive materials has been proposed to prevent caries recurrence.8,9
An acid agent could have an antibacterial effect because of its low pH. Settembrini et al. reported that etchants removed the bacteria on cavity walls.10 However, self-etching adhesive systems do not use acid etching systems. Consequently, a cavity only needs to be air blown and not rinsed with water when these systems are used. That will save clinical chair time but may increase the chances of the survival of the bacteria remaining in the smear layer.
An antibacterial effect is desired for restorative composites and adhesive systems in order to avoid the growth of the remaining bacteria in the cavity. This effect can be achieved by the incorporation of antibacterial agents, such as glutaraldehydes, fluorides, or antibacterial monomers in the formulation of adhesive systems.11-16
In general, adhesive monomers of self-etching adhesive systems present a hydrophilic group at one end of the molecule, which is usually an acid, such as hydrogen phosphate or carboxylate. These traits provide these materials with a low pH and possibly some antibacterial properties. Therefore, not only antibacterial agents but also other substances commonly found in the adhesive system formulas, such as adhesion-promoting monomers that are acidic to different degrees, might exhibit some activity against bacterial growth.17,18
The components of a dentin bonding system are resin-based, like composite resin. It was found that a cured composite did not release any antibacterial components, producing no inhibition halo.17 Therefore, no elution of adequate amounts of antibacterial components from cured composites has been demonstrated. These results are not surprising since the fundamental components of composites exhibit little or no bacteriostatic/bactericidal effects against oral bacteria at low concentrations.
Among the antibacterial agents incorporated into adhesive materials, the resin monomer 12-methacryloyloxy dodecyl-pyridinium bromide, known as MDPB, stands out.8,9,11,12 The main advantage of MDPB is its capacity to copolymerize with other resin monomers that are immobilized within the polymer matrix, which confers safety and prolonged antibacterial action to this agent. Furthermore, it does not leach to the medium. This characteristic also ensures a good survival rate for the restoration, as MDPB, unlike soluble antibacterial agents, is not deleterious to the physical and mechanical properties of the adhesive materials.8,9
Although several studies describe the antibacterial effects of the MDPB monomer, little is known about the antibacterial effects of other self-etching adhesive systems. As the antibacterial effect occurs, other commercially available self-etching adhesive systems could also exhibit this antibacterial effect. This study was conducted to evaluate the antibacterial activity of 2-step and 1-step self-etching systems, with or without light activation, against Streptococcus mutans (S. mutans) by using an agar diffusion test (ADT). The null hypotheses were as follows: 1) There is no difference among inhibition zones, 2) light activation and pH do not influence the inhibition zone, irrespective of the bonding system.
Materials and methods
Bacterial strain and culture
S. mutans ATCC 25175 was used in this study. The bacteria were cultured in a tryptic soy broth (Difco Laboratories, Detroit, MI, USA) at 37℃ aerobically. The culture was started from freeze-dried stocks in 10 mL of a sterile tryptic soy broth. The culture was grown at 37℃ in an incubator (Hi-Tec Model 1S-61, Yamato Scientific Co. Ltd., Tokyo, Japan) for 24 hours.
Preparation of specimens
Three 2-step self-etching systems, Clearfil SE Bond (SE, Kuraray, Okayama, Japan), Contax (CT, DMG, Hamburg, Germany), and Unifil Bond (UnB, GC, Tokyo, Japan), and three 1-step self-etching systems, Easy Bond (EB, 3M ESPE, Saint Paul, MN, USA), U-Bond (UB, Vericom, Anyang, Korea), and All Bond SE (AB, BISCO, Schaumburg, IL, USA) were used for evaluating the antibacterial activity (Table 1). 0.12% chlorhexidine (CHX, Bukwang, Seoul, Korea) and 37% phosphoric acid (PA, Vericom) gel were used as the positive controls. 20 µL of each primer or bonding agent was applied to sterilized paper disks (diameter, 8 mm; thickness, 1.5 mm) with a pipette. A total of 10 specimens were used per group except for the positive and negative controls. Because the number of experimental and control groups was 20 (CHX, PA, three 2-step self-etching systems and three 1-step self-etching systems with or without light activation), the specimens were distributed into four petri dishes. Five paper disks smeared with the self-etching systems, CHX, and PA were placed on each petri dish. Another 20 µL of adhesives were applied and light activated in the case of the 2-step self-etching systems.
Agar diffusion test
The antibacterial activity of each bonding system was evaluated against the S. mutans ATCC 25175. From the culture, bacterial suspensions were prepared in a tryptic soy broth until a turbidity compatible with 0.5 MacFarland was obtained. This scale allowed the bacterial concentration of a suspension to be estimated by its turbidity, 0.5 corresponded to a concentration of 1.5 × 108 (CFU/mL) at an optical density of 550 nm. The specimen disks were placed on tryptic soy agar (Difco Laboratories) plates inoculated with S. mutans. The positive controls of 0.12% CHX and 37% PA gel were added onto the paper disks. The diameter of the inhibition zone produced around each disk was measured after 48 hours of incubation (Figure 1).
Results
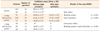
The mean diameters and the standard deviation values of the antibacterial inhibition zones are given in Table 2. Control groups of CHX and PA exhibited the widest zone, 28.43 ± 0.59 mm and 27.27 ± 1.11 mm each. The inhibition zones of 2-step self-etching systems SE, UnB, and CT were 26.66 ± 0.27 mm, 21.61 ± 0.35 mm, and 10.58 ± 0.35 mm, respectively, when they were applied without light activation, while their zones became narrow in the order of SE (24.81 ± 2.22 mm), UnB (17.41 ± 0.26 mm), and CT (10.76 ± 0.48 mm). The inhibition zones of 1-step self-etching systems EB and UB were 10.87 ± 1.07 mm and 18.65 ± 0.49 mm, respectively, when they were uncured. However, these zones could not be formed when they were cured. The other 1-step self-etching system AB did not form any inhibition zone, irrespective of the light activation.
Two-way ANOVA indicated significant differences for the 'materials' (p = 0.000) and 'light activation' (p = 0.000) factors and for the interaction between the factors (p = 0.000) (Table 2). The positive CHX control group exhibited the most effective antibacterial activity against S. mutans, and the PA group was the next. Among the experimental groups, SE was the most effective, and its inhibition zone did not differ from that of the 37% PA positive group (Figure 1). All 2-step self-etching systems showed various inhibition zones with and without light activation. Light activation diminished the inhibition zone except in the case of CT. In contrast, all 1-step self-etching systems did not exhibit any antibacterial activity after light activation on the adhesive. EB and UB showed an inhibition zone when the agent remained in situ without light activation. However, the antibacterial effect vanished upon light activation. No inhibition zone was detected in the case of AB both with and without the light activation.
Discussion
ADT was used because it is a widely employed methodology for the determination of the inhibitory activity of liquid substances, in addition to being a simple and easy-to-handle technique and facilitating the comparison to other studies.19 The advantage of this method is that it allows direct comparisons of test materials against the test microorganisms, indicating which test materials have the potential to eliminate bacteria in the local microenvironment. Further, the results of ADT can indicate the existence of diffusible components into an aqueous milieu.
However, ADT has limitations in that it measures only the water-soluble components and the solubility and the diffusability of the test agent affect the inhibition zone.20 The results of this method do not depend only on the toxicity of the material for a particular microorganism but are also highly influenced by the diffusability of the material across the medium. A material that diffuses more easily will probably provide larger zones of microbial growth inhibition.21,22 Other variables such as inoculum size, incubation time, and the material/agar contact may also affect the results.
S. mutans colonization on tooth surfaces has been recognized in the etiology and pathogenesis of human dental caries.23 The ability of S. mutans to produce acid by sugar fermentation and its capacity for acid tolerance comprise key virulence factors involved in the development of dental caries.24 Acid production by S. mutans leads to low pH values in dental plaque and contributes to the demineralization of tooth enamel and initiation of caries formation.25 Accompanying the acidogenicity of S. mutans is its acid-tolerance or aciduricity. S. mutans maintains glycolytic capabilities even at pH 4.4, the level that is growth-inhibitory.26 S. mutans resists environmental acid stress by increasing the proton translocating F-ATPase activity in response to a low pH.27 This mechanism makes the intracellular pH more alkaline than the extracellular environment pH, which plays a critical role in the pathogenesis of dental caries.28
There are several studies that describe the bonding system incorporating antibacterial components. Bapna et al. studied the antibacterial activity of the Scotchbond adhesive resin to which various chemical agents were added.29 Although their study was not oriented to develop an antibacterial bonding system, cured resins containing sodium fluoride, dodecylamine, or bipyridine inhibited the growth and attachment of S. mutans. Kudou et al. attempted the incorporation of vancomycin or metronidazol to a 4-META/MMA-TBB resin in order to develop an antibacterial bonding system for direct pulp capping.30 They reported that the resin containing 1 - 5% vancomycin produced inhibition against all streptococci and actinomycetes tested, and the resin with vancomycin did not affect the tensile bond strength. Imazato et al. investigated the utilization of 5% MDPB with the self-etching adhesive system (Clearfil Protect Bond) against S. mutans, Lactobacillus casei, and Actinomyces naeslundii.12 As unpolymerized MDPB exhibits strong bactericidal activity, the residual bacteria in the cavity can be inactivated when a MDPB-containing bonding system is applied. Further, the bacteria can be inhibited by the immobilized agent after light activation as in the case of the surface of MDPB-added composites. Therefore, by the incorporation of MDPB, a bonding system with antibacterial effects before and after setting can be achieved.
The current findings demonstrate the different inhibition levels produced by different 2-step self-etching systems or 1-step self-etching systems. As speculated earlier, the main reasons for the inhibition of bacterial growth are probably the cytotoxicity of the monomer or the acidic pH of the self-etching primer.13 However, Imazato and Feuerstein et al. suggested that the benefit of a low pH environment exhibited by dentin bonding systems should be considered to be 'limited'.17,31
It was presumed that a relatively low pH affected the inhibition zone. However, this no longer seems to be an important influential factor because of the small pH difference among systems considered in this study. In spite of the acidic nature of self-etching adhesive systems, this characteristic does not seem to be sufficient to completely eliminate the residual bacteria from dentin because this tissue acts as a solid buffering medium to acidic monomers.32
2-methacryloyloxy ethyl phenyl hydrogen phosphate (Phenyl-P), 4-methacryloyloxyethyl trimellitate anhydride (4-META), and 10-methacryloyloxydecyl dihydrogen phosphate (MDP) are the main acidic monomers contained in the formulation of self-etching adhesive systems and are capable of demineralizing and infiltrating the dentin substrate simultaneously. According to Ohmori et al., MDP has a higher inhibitory function against microorganisms than Phenyl-P.18 MDP is present in both the primer and the adhesive components of SE, which exhibited the best results among the experimental groups in this study.
The inhibition of caries associated with bacteria was observed when the uncured specimens were tested, but the antibacterial effects were adversely affected by the curing. The polymerization of adhesive materials causes entrapment in the polymeric matrix and decreases the release of polymerizable antibacterial components, as well as adhesion-promoting acidic monomers.33 Nevertheless, even in the case of light activation, there was some antibacterial activity when the 2-step self-etching systems were applied to the paper disks. The formation of the zones of microbial growth inhibition when the adhesive systems were light-activated may be explained by the fact that a complete conversion of monomers into polymers does not occur and hence, residual monomers can be released to the medium.34 Furthermore, light is not capable of passing through a paper disk that is adequately impregnated with the adhesive components.33 The antibacterial effect might also be due to the release of the residual monomers present in the oxygen-inhibited layer.35
The methodology employed in the present study has some limitations with respect to the reproduction of the physiological conditions of the pulpo-dentinal complex, such as the presence of intratubular fluid and intra-pulpal pressure. Due to these limitations, the results obtained in in vitro studies cannot be directly extrapolated to an in vivo situation because they may not reflect the actual effect of the material when applied under clinical conditions. However, laboratory tests are indispensable because they are at the base of the scientific evidence pyramid providing research-based support and serving as a reference for clinical investigations. Therefore, although the present study demonstrated in vitro the antibacterial characteristics of some self-etching systems with and without light activation, further clinical trials should be conducted to determine the inhibitory effect of bonding systems against cariogenic microorganisms. Moreover, other methods, such as the direct contact test and aging test, should be considered to compensate for the drawbacks of ADT.
Conclusions
In this study, we found that the antibacterial activity of CHX and PA was higher than that of the other experimental groups, except the SE primer. Among the self-etching systems considered, SE exhibited the most effective antibacterial activity against S. mutans. After light activation, the inhibition zone was reduced in the case of all 2-step self-etching systems except CT. 1-step self-etching systems, such as AB, EB, and UB, did not exhibit the formation of any inhibition zone upon light activation.


 XML Download
XML Download