

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
During the past decade, zirconia ceramic technology has led to rapid advances in metal-free dentistry.1 Unique properties of yttrium oxide (yttrium-tetragonal zirconia polycrystal, Y-TZP), namely its flexural strength of 1,000 MPa, chemical stability, biocompatibility and optical properties, have made Y-TZP a good choice for the fabrication of all-ceramic crowns, long-span bridges, posts and cores and implants.2,3,4,5 Zirconium oxide crowns can be cemented using conventional and adhesive techniques.6,7
Previous studies have shown that indirect all-ceramic restorations require a durable bond between the cement and the ceramic for longevity.8,9,10,11 Use of resin cements improves retention, fracture resistance and the marginal adaptation of the restoration to the tooth structures.10,12 It has been reported that use of adhesive resin cements containing phosphate monomers may contribute to bonding of zirconia restorations to tooth structures.13,14,15
There is no consensus for achieving optimal bond strength between composite resins and zirconia. Zirconia ceramics have a highly crystalline structure. Therefore, achieving a proper micromechanical bond between the resin cement and zirconia ceramic restoration with routine preparation techniques, including acid etching with hydrofluoric acid, is considered an ineffective method.9,16 Other techniques have been suggested for surface treatment, including surface abrasion, sandblasting, abrasion with diamond burs, air abrasion with aluminum oxide, silicoating, and selective infiltration etching.17,18 Recently, due to advances in laser techniques, some studies have suggested application of lasers such as CO2, Er:YAG and Nd:YAG to bring about changes on zirconia ceramics to improve their bond to tooth structures.12,17,19,20 Some studies have shown that use of CO2 and Er:YAG lasers improves the bond strength to zirconia ceramics.12,17,19,20 However, some studies have yielded contradictory results.20,21,22
The aim of the present study was to evaluate and compare the effects of CO2 and Er:YAG lasers on the shear bond strength of resin cement to zirconia ceramic. Based on the null hypothesis of this study, pretreatment of the zirconia ceramic surface with CO2 and Er:YAG lasers has no effect on shear bond strength of resin cement to zirconia ceramic.
Materials and Methods
The present in vitro study was performed on 45 zirconia disks. Presintered zirconia cylinders (9.8 mm in diameter and 20 mm in height, Ceramill Zi, Amann Girrbach AG, Koblach, Austria) were prepared by a milling machine (Ceramill, Multix, Amann Girrbach AG) and copy milling technique based on the manufacturer's instructions to obtain specimens with a dimension of 2.5 mm in diameter and 7.5 mm in height (Table 1). Next, the specimens were densely sintered in a furnace (Sirona Dental Systems LLC, Charlotte, NC, USA) under the conditions (1,530℃ for 1 hour and cooling for 6 hours) suggested by the manufacturer using the proprietary sintering program (Amann Girrbach AG). The discoid-specimen size after sintering was 6 mm in diameter and 2 mm in thickness. The specimen surfaces were treated with airborne particle abrasion with 50 µm Al2O3 at 2-bar pressure and were polished by hand with 600-grit silicon carbide paper (Matador 991A, Soflex, Starcke GmbH & Co. KG, Melle, Germany) to standardize them.
All the specimen surfaces were treated with airborne particle abrasion with 50 µm Al2O3 at 2-bar pressure and were wet polished by hand with 600-grit silicon carbide paper (Matador 991A, Soflex, Starcke GmbH & Co. KG) to standardize them. The surfaces of sintered zirconia disks were observed by ×2.5 loop, and samples with surface cracks or voids were replaced by new ones. The specimens were cleaned in an ultrasonic bath containing isopropanol for 3 minutes and dried by air syringe before surface treatment and then were randomly assigned to 3 groups of 15:
CNT group: No surface pretreatment was applied in this group (control).
COL group: The bonding surfaces of zirconia disks were irradiated by CO2 laser (Smart US 20D, Deka, Florence, Italy). Laser beam parameters were selected based on the results of previous studies for micromechanical retention.17,19,21,23 The wavelength of CO2 laser was 10.6 µm, with a pulse repetition of 100 Hz, pulse duration of 160 ms, output energy of 3W and energy density of 265.39 J/cm2. Laser was delivered by a 600 µm hollow ceramic tip that was hand-adjusted perpendicular to the ceramic surface at a distance of approximately 1 mm. Laser beam diameter at the irradiated surface was 0.48 mm. The whole surface of the zirconia disk, measuring 6 mm in diameter (0.28 cm2), was irradiated for 10 seconds at a rate of 2 mm/s using horizontal surface scanning mode.17,19,21
EYL group: The surfaces of zirconia disks were covered with graphite powder to increase laser energy absorption and irradiated with Er:YAG laser (Fidelis Plus III, Fotona, Ljubljana, Slovenia). Laser parameters were set as follows: wavelength of 2,940 nm, pulse duration of 50 µs (SSP), output power of 2 W, pulse repetition of 10 Hz and energy density of 200 mJ, using R14 handpiece and an 800 µm sapphire tip, with water/air spray ratio of 4/4. The sapphire tip was adjusted by hand at an approximate distance of 0.5 mm, perpendicular to the disk surface and the entire zirconia disk surface (0.28 cm2), was irradiated at a rate of 2 mm/s for 10 seconds using horizontal surface scanning mode.12,19
One additional specimen from each group was prepared and sputter-coated with gold for evaluation of micromorphology of the zirconia surface. The samples were analyzed using scanning electron microscope (JSM-6335F, JEOL, Tokyo, Japan) at ×1,000 and ×5,000 magnifications.
Composite resin disks (Filtek Z 250, 3M ESPE, St. Paul, MN, USA), 3 mm in diameter and 2 mm in thickness, were fabricated by packing composite resin in one increment into transparent plastic molds placed on glass slabs followed by light-curing for 40 seconds at a distance of 1 mm using a light-curing unit (Demi, Kerr Corporation, Middleton, WI, USA) with 1,000 mW/cm2 intensity. The composite resin disks were cemented to the surface of zirconia samples using a dual-curing resin cement (Panavia F2.0, Kuraray Noritake Dental Inc., Osaka, Japan). First, the primers A and B were admixed and then applied to the surface of ceramic and composite resin with a microbrush. After 20 seconds, the resin cement tubes A and B were mixed and placed between ceramic disks and composite resin and each composite resin disk was bonded to a zirconia disk by finger pressure.17,20,21 Excess cement was eliminated and the specimens were light-cured for 20 seconds. Finally, the specimens were rinsed with air and water spray and stored in distilled water at 37℃ for 24 hours before shear bond strength testing. The shear bond strength test was performed in a universal mechanical testing machine (Dartec HC10, Dartec Ltd., Stourbridge, England) at a strain rate of 0.5 mm/s.
All the fractured samples were evaluated twice under a stereomicroscope (SZ40, Olympus, Tokyo, Japan) at ×40 magnification for fracture modes (cohesive, adhesive and mixed) by one operator. Data were analyzed by SPSS 13, using one-way ANOVA and post-hoc Tukey's HSD tests. Statistical analysis was set at a confidence interval of 0.95%, power of 80% and a significance level of p < 0.05.
Results
The highest (12.12 ± 3.02 MPa) and lowest (5.97 ± 1.14 MPa) mean shear bond strength values were observed in the COL and CNT groups, respectively. The mean shear bond strength value in the EYL group was 8.65 ± 1.77 MPa (Table 2). One-way ANOVA showed statistically significant differences in shear bond strength values between the three groups. Pairwise comparison of the groups by post-hoc Tukey's tests showed significant differences between all groups (Table 2).
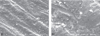
Evaluation of the mode of failure in groups showed that 100% of the fractures in the CNT group were adhesive (between zirconia and cement). However, in the COL and EYL groups, 80% of the failures were adhesive and 20% were mixed (between the composite resin and resin cement) (Table 2). The SEM photograph of zirconia ceramic surface treated with CO2 and Er:YAG laser under an electron microscope at ×1,000 and ×5,000 magnifications showed that application of 3W CO2 laser beam to the surface of zirconia produced cracks on the ceramic surface. Surface pretreatment by Er:YAG laser enhanced surface roughness with a scaly appearance (Figures 1, 2, 3).
Discussion
Considering current advances in laser technology, laser beam irradiation is used in various dental procedures, including roughening the surface of ceramics. In the present study, the effects of Er:YAG and CO2 lasers on shear bond strength of resin cement to zirconia ceramic were evaluated and compared. In this study, in both case and control groups, Panavia cement which has ester phosphate monomer (10-methacryloyloxydecyl dihydrogen phosphate: MDP) was used, because there has been numerous evidences showing that the bonding to Y-TZP ceramics will be improved by using products having chemical affinity to metal oxides.24,25 Ester phosphate monomers such as MDP have chemical reaction with zirconium oxide and form a strong bond with zirconia ceramics.26 The results of the present study clearly showed that surface preparation with CO2 and Er:YAG lasers increased the shear bond strength of resin cement to zirconia surface (p < 0.001). Therefore, the null hypothesis of the study was refuted. Consistent with the results of the present study, some previous studies have also shown that CO2 and Er:YAG lasers can increase the shear bond strength of resin cement to zirconia without aging method and after thermocycling.12,17,19,23,27,28
Zirconia ceramic can completely absorb the energy of the CO2 laser beam. After absorption of laser energy, a process called heat induction produces shell-like ruptures on the ceramic surface, which can provide a micromechanical bond between the resin material and the ceramic surface after resin tags penetrate into these cracks and set.17,28 Micromorphologic evaluation of the surface of ceramics has shown that the CO2 laser produces a rough surface with a scaly appearance and microcracks.12,17,28 The micrograph of the zirconia disc surface in our study also showed scaly appearance and microcracks (Figure 2). Akyil et al. showed that treatment of zirconia surfaces by CO2 laser at power of 4 W resulted in microcrack, scaly appearance and significantly increased bond strength of resin cement to zirconia.19 It seems that resin penetration to microcracks leads to increased bond strength of resin cement to zirconia; however weakening the sub surface of zirconia could affect the mode of fracture.
Er:YAG is not absorbed as well as the CO2 laser by the zirconia surface. Thus, in order to enhance its absorption, we covered the ceramic surface with graphite powder. As seen on SEM images (Figure 3), Er:YAG laser increased surface roughness without causing microcracks on the zirconia ceramic surface and significantly increased the resin cement bond strength (p = 0.004). Previous studies have demonstrated that Er:YAG laser produces a rough surface.12,29,30 Akin et al. reported that irradiation of a lower power Er:YAG laser at 150 mJ, 10 Hz, 1 W and long pulse for 20 seconds on Y-TZP ceramic material enhanced the surface roughness without microcrack formation on the ceramic surface.27 In contrast, some studies have shown that irradiation of zirconia ceramic surfaces with CO2 and Er:YAG lasers does not result in an increase in shear bond strength of resin cement to pretreated surfaces.20,22,28,29,31 This discrepancy in results may be attributed to differences in surface laser pretreatment methods. Absorption of the laser beam energy by the material surface is the most important interaction (the thermomechnical effect) between the laser and the material.12 Increase in output energy and pulse rate of the laser beam results in increasing the energy density and thermal effects on the surface. In pulsed lasers such as Er:YAG laser, changing the pulse duration changes the peak power and its effects on the material surface.
Foxton et al. reported that Er:YAG laser decreased the shear bond strength between zirconia cement and resin cement.22 They used Er:YAG laser beam with 10 mJ/pulse and 200 Hz for 5 seconds; pulse duration was not reported in their study. However, in the present study, the Er:YAG laser beam parameters were 10 mJ/pulse, 200 Hz, and pulse duration of 50 µs for 10 seconds. In the present study, the newer technology of Er:YAG laser with a pulse duration of 50 µs was used. This low pulse duration increased the laser power peak, thus, increasing the effect of the laser energy on the surface. Lin et al. reported that Er:YAG laser had no effect on zirconia surface at different laser energy intensities (100, 200 and 300 mJ) and irradiation times (5, 10 and 15 seconds).29 In contrast to the present study, they did not use graphite powder to increase absorption of laser energy by zirconia. Coating the surface with graphite powder increases the absorption of laser energy by the white opaque zirconia ceramic.
Contrary to the results of the present study, Akin et al. reported that Er:YAG laser significantly increased the bond strength of resin cement to zirconia more than the CO2 laser. They reported smooth surfaces on CO2 laser-treated zirconia samples with no retention.21 These results may be attributed to the low energy density of the CO2 laser beam (159.22 J/cm2) in their study. In our study, despite the low energy level of the CO2 laser beam (3 W), the energy density of the laser beam was higher (265.39 J/cm2) considering the diameter of the laser beam delivered, which resulted in a rough surface due to its thermal effects. The rough surface was clearly seen in SEM micrographs (Figures 1 and 2). Scaly irregularities on the zirconia surface increase micromechanical retention and improve shear bond strength of resin cement to the zirconia surface.
Pretreatment of zirconia surface with CO2 laser resulted in a greater increase in bond strength values compared to the Er:YAG laser (p < 0.001) in the present study, which can be attributed to the extent and type of the surface irregularities produced on the zirconia surface. Microcracks produced by the irradiation of the zirconia surface with CO2 laser were visible in different areas of the surface on SEM micrographs while no microcracks were observed on the surfaces exposed to Er:YAG laser beam. A higher bond strength with the use of CO2 laser may be attributed to better absorption of CO2 laser compared to Er:YAG by the zirconia surface resulting in more surface roughness. Surface microcracks facilitate the penetration of resin tags and cement into such an irregular surface and improve adhesion. Profilometric evaluations are necessary to evaluate surface irregularities produced by laser beams on zirconia surfaces, which is one of the limitations of the present study. Consistent with the results of the present study, Akiyl et al. reported that preparation of zirconia surface with CO2 laser resulted in a greater increase in shear bond strength of resin cement to this surface, compared to Er:YAG laser.19
Evaluation of fracture modes in the present study showed that 100% of fractures were adhesive in the control group. In the COL and EYL groups, 20% of the fractures were mixed. In other words, there was an increase in the frequency of mixed failures at the zirconia surface-resin cement interface with an increase in shear bond strength values, consistent with the results of some previous studies.20,21,32 Apart from the bond strength between the resin cement and zirconia surface, the durability of the bond is more important for the clinical success of restorations.




 XML Download
XML Download