

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Single-tooth replacement in the anterior region presents a challenge for the clinician. In this region, treatment considerations include shape and shade matching of the crown, interdental spacing, topography of the ridge, contacts of the opposing dentition, parafunctional habits, and esthetic desires of the patient.1 Various treatment options can be considered for the replacement of a traumatically missing permanent incisor. For many years, the fixed dental prosthesis has been the treatment of choice for this purpose. However, it requires aggressive tooth reduction, which may increase the possibility of endodontic treatments. The development of implant-supported prostheses has enabled a more conservative approach. However, the need for surgical procedures and its high cost may reduce its accessibility for some patients. Further, it is difficult to obtain a natural-looking appearance if the tooth alignment is not appropriate.
During the last decade, fiber-reinforced composite (FRC) was suggested as an alternative material for restorations. Properties of FRC, such as strength, desirable esthetic characteristics, ease of use, adaptability of various shapes, and potential for direct bonding to tooth structure make it suitable for various applications.2,3 Therefore, alternative treatment using FRC has been reported to replace a single anterior tooth when conventional treatment options are not indicated, such as in the case of implant treatment when the patient is anxious about the surgical process or fixed partial prosthesis with excessive removal of the tooth structure.4,6,7 This case report describes a clinical case that utilizes the FRC fixed partial prosthesis with direct composite build-up as an alternative solution for replacing the missing single anterior tooth.
Case report
A 44-year-old woman visited the Department of Conservative Dentistry because of tooth avulsion of the left maxillary central incisors after an injury caused by falling down one day before visiting the dental office. The patient brought the avulsed tooth wrapped in tissue paper. The tooth was totally dry. Clinical and radiographic examination revealed that tooth #21 was avulsed, and a blood clot was found in the alveolar socket (Figure 1). Debridement of the contaminated root surfaces, endodontic treatment, and resin-wire splint were performed. At the 8-week recall, mobility of tooth #21 had increased and periapical radiographs revealed that there was an obvious radiolucent band around the root surface (Figure 2). It was diagnosed as a failure of replantation on #21. The patient was referred to the Department of Prosthodontics for further treatment. However, the patient did not show up for 10 months for personal reasons.
One year after the trauma, the patient came to our department again for checkups. The patient was free of symptoms, and #21 was retained by a lingual fixed retainer, which was made at a local clinic. Clinical examination showed a gingival recession of about 4 mm on #21 and full probing depth around #21. Additionally, a black triangle was formed between #11 and #21 (Figure 3). The patient complained about the conventional treatment options and refused both conventional fixed partial prosthesis and implant restoration. In case of treatment with conventional fixed partial prosthesis, excessive preparation of the adjacent tooth was necessary for crowding relief, and additional endodontic treatment was required. She refused this option because of the tooth preparation of the adjacent teeth. When we considered an implant, additional bone graft was necessary due to the loss of the buccal plate in the extraction socket area. In addition, she was anxious about implant treatment due to past experience during implant surgery on the left mandibular second molar. Also, due to crowding on the left maxillary lateral incisor, implant placement was particularly difficult. After discussing all treatment options with the patient, the FRC fixed partial prosthesis was chosen. An impression was made with alginate for the FRC fixed partial prosthesis fabrication. It was possible to avoid occlusal stress on restoration because the avulsed tooth was out of contact (Figure 4).
After local anesthetizing the area, the tooth was extracted. A piece of sterile gauze was gently packed into the extraction site to prevent bleeding. After hemostasis, the prefabricated temporary composite crown was held in position attached to the adjacent teeth with direct composite, and then, the interproximal gingival contour was reformed (Figure 5).
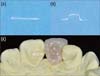
Thirty minutes before the patient's next visit, a composite pontic was fabricated using nanofilled composite (Filtek Z350 XT, 3M ESPE, St Paul, MN, USA) to enhance the cohesion between the lab-fabricated pontic and the intraoral direct-filled composite. The fiber framework (FibreKor, Jeneric/Pentron Inc., Wallingford, CA, USA) was cut to the appropriate length and adapted to the abutment teeth and the pontic area. The framework was covered with a body layer of the pontic and light polymerized. The FRC framework was located in the palatal 1/3 area of #11 and #21, and in the buccal 1/3 area of #21 pontic (Figure 6).
When the patient arrived, the abutment teeth were anesthetized and the temporary composite crown was removed (Figure 7). The abutment teeth were prepared using tapered diamond burs (835.31.009, Brasseler, Savannah, GA, USA). The preparations consisted of removing approximately 1.0 mm of the lingual surface of the abutment teeth to ensure adequate space for the placement of the fibers and composite resin. All margins were in enamel (Figure 8). After the preparation, a 37% phosphoric acid gel (ETCH-37, Bisco Inc., Schaumburg, IL, USA) was applied to the enamel margin for 20 seconds. The etchant was thoroughly rinsed off and gently dried. Clearfil SE bond (Kuraray Medical Inc., Tokyo, Japan) was applied following the manufacturer's instructions, and a thin layer of flowable composite resin was placed on the prepared surfaces of the abutment teeth. The prefabricated FRC fixed partial prosthesis (Figure 9) was inserted in the cavity. Fiber was pressed into the unpolymerized flowable composite resin (Aelite Flow, Bisco Inc.) using a hand instrument and cured for 20 seconds. The exposed fiber surfaces on the abutment teeth were covered with Filtek Z350 XT and cured for 40 seconds (Figure 10). Composite was added to the pontic in order to obtain a more natural shape and shade of the final restoration and to reinforce the connector area of the interproximal surface. Occlusal adjustment was made using articulating paper and diamond finishing burs, and surfaces were polished with Soflex (3M ESPE) (Figure 11).
At the 1-year recall, the patient stated that she was satisfied with the appearance and function of the prosthesis. The pontic area and resin-bonded margins were clinically sound, and the abutment teeth were intact (Figure 12). The pontic was in good condition, and the desired shade of the teeth had been maintained.
Discussion
FibreKor is composed of a polymer matrix impregnated with unidirectional glass fibers, 8.0 µm in diameter, with an elastic modulus of 22 - 27 GPa. This structure allows the FRC to be placed easily on a tooth surface with minimal thickness and increased bonding surface area of contact between the FRC and the etched enamel.8 Furthermore, materials that have an elastic modulus similar to dentin (18.6 GPa) may enhance the clinical longevity of restorations because the FRC framework provides a more balanced and even stress distribution.
Maximum stress concentrations were located in the connectors in FRC fixed partial prosthesis and metal framework fixed partial prosthesis.9 The dimension of the connector was 4 (inciso-gingivally) × over 2 mm (labio-lingually) to resist the occluding forces. However, esthetic aspects should be considered in addition to the functional aspects for restorations in the maxillary anterior region. In most cases, the optimal placement of the interproximal connector is on the incisal or middle third of the tooth. This location mimics the presence of the interproximal contact area between adjacent teeth and provides access for the clinician to shape the restoration and reestablish an esthetic result. The management of the embrasures, facial interproximal connector areas, and the gingival embrasures is important to achieve desirable esthetics and function. In this case, the interproximial area of #21 and #22 overlapped, and the contact surface area was larger than the mesial surface area. We, therefore, tried to expand the connector area as much as possible without compromising the esthetic result. There was a black triangle between #11 and #21. However, expanding the connector surface longitudinally to cover the black triangle would lead to a poor esthetic result. Therefore, following Salama's study, the contact point was modified to induce gingival growth longitudinally.10
When selecting the retainer type for an FRC fixed partial prosthesis, mechanical and biologic aspects must be considered. An FRC fixed partial prosthesis may be retained using complete-coverage crowns, inlays, surface-retained wings, or their combinations. The use of full-coverage retainers suggested a high survival rate. However, the required preparations are as extensive as those required for conventional fixed partial prosthesis.11 Jain and Cobb suggested similar survival rates for inlay-retained FRC fixed partial prosthesis.12 Additionally, Vallittu showed that an inlay-retained FRC fixed partial prosthesis had better survival rates than a surface-retained prosthesis.13 Thus, inlay-retained FRC was used to minimize the need for tooth preparation and to provide long-term success. At the same time, the margins were located within the enamel for better marginal adaptation.
Most previous clinical studies fabricated FRC fixed partial prosthesis by using an extracted tooth in pontic and direct intraoral application techniques. A patient's own tooth can be used as pontic if the extracted tooth has no esthetic problems. However, in this case, the crown shape of the two adjacent teeth was different (#21 was triangular, and #11 was oval), and there was malalignment of the anterior teeth due to labioversion of #21 (Figure 4). To solve these esthetic problems, the pontic was built up with composite instead of an extracted tooth (Figure 11b). Moreover, direct application of the fiber framework and building up composite resin pontic are complex and time-consuming techniques. Polishing the gingival surface of the pontic on the finished FRC fixed partial prosthesis is not easy. In order to overcome this shortcoming, some authors have tried to simplify the manufacturing process by developing a modified technique called the 'semi-direct technique'.14 Therefore, in this case, the build-up procedure for the pontic was carried out with a replicated model up to the body layer. Then, the pontic was moved to the patient's oral cavity and bonded to the tooth cavity. The pontic's enamel layer was formed in balance with the patient's adjacent tooth shade and shape. In this chair-side step, adjustment of the interproximal contact and the contact area was accomplished.
Despite such efforts, there are some limitations in this case. When we were planning the treatment, ridge augmentation was suggested to the patient for better esthetic result considering the gingival contour of #21. However, she rejected our suggestion because of the additional cost and anxiety about the surgical procedure. The fact that soft tissue management was not carried out influenced the shape of the pontic. Many studies have shown that an ovate pontic design produces the most esthetic result. However, in this case, sufficient recovery of the soft tissue for an ovate pontic was not expected. The gingival tissue under the pontic was depressed slightly as compared with that under the adjacent teeth and formed light contact with the pontic. Although the patient was satisfied with the final restorations, ridge augmentation might be helpful for a better gingival appearance. The longevity of the FRC fixed prosthesis is also threatened by debonding, discoloration, and wear of the occlusal surface made from a veneering composite, in contrast to the metal framework. Thus, case selection plays a great role in the longevity of the prosthesis. It should be emphasized that the FRC prosthesis is not a complete substitute for the conventional fixed prosthesis in all cases.
Conclusions
The technique using a fiber framework and composite pontic, as described in this paper, is a minimally invasive, esthetic, and cost-effective method for the treatment of a single missing anterior tooth. When anterior teeth are restored using FRC, thorough treatment planning is essential to fulfill the need for durable restoration without compromising esthetic results. Therefore, the clinician must design the tooth preparation and subsequent restoration, taking into account the framework, pontic, and the connectors.











 XML Download
XML Download