

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A few surveys of general dental practitioners have been conducted to determine the various factors associated with a referral to an endodontist.1,2,3,4,5 One of these surveys demonstrated the various aspects regarding the relationships between general practitioners and endodontists, such as communication, location, patient management, and waiting time, influenced decisions pertaining to endodontic referrals.2 Following up on patient records, referring patients back for restorative treatment, and accommodating patient schedules were suggested as effective methods in order to build relationships between general practitioners and endodontists.1
Another survey showed that general practitioners considered clinical factors such as presence of a perforation, resorption, persistent signs, and persistent symptoms, to be important for endodontic referrals.3 Surveys of general practitioners reported various endodontic problems, demonstrating that a referral to an endodontist depends on the potential procedural difficulty that may occur during endodontic treatment.4,5 However, the prevalence of specific endodontic problems that occur in a general practitioner's clinic may differ from that of the perceived endodontic treatment difficulty.
Management of pain, calcified/blocked canals, and endodontic retreatment were shown to be the main reasons in a study of clinical records conducted to investigate the reasons for endodontic referrals.6 In more recent studies, the main motive for an endodontic referral was the questionable clinical status to support the retention or extraction of a tooth.7,8,9 Besides these studies, little information exists in order to investigate the prevalence and nature of endodontic conditions. In addition to the American Association of Endodontists (AAE)'s endodontic case difficulty assessment guidelines, information regarding the prevalence of endodontic difficulties that occur frequently will help general practitioners identify cases that require prompt referral.10
In Korea, many patients are willing to go to an endodontist at a general hospital level in order to save the tooth that has an endodontic problem. It is because endodontic treatment fees are covered by the National Health Insurance system, and accessibility to general hospitals is adequate. Consequently, patients can be easily referred to endodontists to receive treatment for teeth that have endodontic difficulties. Most patients are referred with the goal of saving their teeth per their wishes following a general practitioner's diagnosis.
This study aimed to investigate the prevalence of endodontic problems that led to a referral, and the clinical symptoms that were perceived to be difficult for general practitioners to handle in Korea.
Materials and Methods
Clinical data regarding the total number of endodontically treated cases, as well as the total number of endodontic referrals, from January 1, 2010, to December 31, 2012, at Kangdong Sacred Heart Hospital, Seoul, Korea, were investigated retrospectively. The endodontic cases were considered referrals for the purposes of this study if other dental clinics had referred patients to endodontists at this hospital. Cases referred from the specialists at the same hospital, such as prosthodontists, orthodontists, oral surgeons, and postgraduate students, were excluded from the endodontic referrals in this study.
The primary reasons for endodontic referrals were recorded in an interview with the patients according to the comments of patients, and the comments in the referral documents from the referring dentists irrespective of clinical states of the tooth. If more than one reason existed, only the reason that was considered the major problem was recorded.
In this study, the author investigated clinical symptoms such as presence of pain, apical radiolucency, previous endodontic treatment, gingival swelling and sinus tract, and other clinical problems by using a direct examination, a chart review, and periapical radiographic images. As most cases had more than one symptom, all presenting symptoms were recorded separately from that of primary reason for referral. The percentages of clinical symptoms of the endodontic referral cases and the total endodontic treatment cases were compared by χ2 test for each symptom, and significance was set at 5% probability level.
Procedures that were performed to resolve the conditions justifying the referrals were investigated. Endodontic treatments were performed by the author, and incisions and drainage of pus for relief of acute symptoms prior to an endodontic treatment were performed in the oral and maxillofacial surgery department. The study design was approved by the institutional review board of the Kangdong Sacred Heart Hospital (IRB N0. 13-2-32), which waived the requirement for patient consent.
Results
A total of 1,014 cases were endodontically treated during the period, and of those, 224 cases were included as the endodontic referrals. Among the endodontic referrals, 129 (57.6%) were female, while 95 (42.4%) were male. The patients in their 50s showed the highest age group (21.9%), while other age groups spread as 20s (16.1%), 30s (18.3%), 40s (16.5%), and 60s (14.7%). The most frequently referred teeth were the mandibular and maxillary first molars, followed by the mandibular second molars.
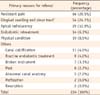
The primary reasons for referral are summarized in Table 1. Endodontic difficulties such as canal calcification, presence of post, broken instrument, perforation, resorption, and other endodontic difficulties were grouped into an 'Others' category. If pregnancy was the primary reason for an endodontic referral, the cases were categorized as having a 'physical condition', which included hypertension, diabetes, cancer, and a physical disability.
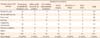
Table 2 shows a comparison of clinical symptoms for the endodontic referrals as well as for all the endodontic cases. The percentages of the presence of pain, apical radiolucency, previous treatment, and gingival swelling and sinus tract for the endodontic referrals were significantly higher than those of all the endodontic cases (p = 0.001)
Treatment procedures that were performed to resolve the referral issue are described in Table 3. Among the 224 patients, 14 discontinued the treatment, while 9 underwent extraction or did not obtain complete resolution of their problem. 72.8% of the cases were treated with nonsurgical endodontic treatment only to resolve their referral problem. 5.8% of the referrals showed that the tooth other than the referred tooth to be diagnosed as the origin of the problem.
Discussion
This observational study attempted to investigate the prevalence of referral reasons and the clinical symptoms of endodontic referrals. In this study, referrals from other specialists such as prosthodontists, orthodontists, and oral surgeons were excluded in order to focus on the reasons for referrals that general practitioners consider as endodontic difficulties, as well as to focus on what influences general practitioners' decision to refer patients to specialists.
Pain was also the main motive for an endodontic referral in the previous studies, but the presence of apical radiolucency and gingival swelling and sinus tract were not analyzed individually.6,7,8 Although symptoms such as presence of apical radiolucency and gingival swelling and sinus tract were simultaneously demonstrated in the referred teeth, one of these symptoms could be considered as the primary reason for referral in the patients who presented in this study. These symptoms were also demonstrated to be the major reasons that general practitioners decide to refer the patient to an endodontist.
Endodontic difficulties such as canal calcification, broken instruments, post presence, perforation, and resorption were grouped because the prevalence of endodontic referrals for these issues was low in this study. General practitioners considered the presence of an obstruction, a perforation, and resorption as the major factor for endodontic referral in prior studies.3,11 These endodontic difficulties are critical regarding treatment failure for a routine root canal therapy, but the actual incidence of instrument fracture and perforation is not high.12,13 Given the actual low incidence, consideration of extraction before referral to an endodontist may also contribute to the low prevalence of endodontic referrals in this study.
Pain, apical radiolucency, previous endodontic treatment, and gingival swelling and sinus tract were the major clinical symptoms of the endodontic referrals, and the percentages of these symptoms were significantly high in this study. As these clinical symptoms present with progression of inflammation of the pulp and periapical tissue, it may be best to refer such cases to an endodontist. Retreatment in failed cases was also strongly recommend to be referred to an endodontist in previous study.11
The treatment procedures that were performed on the endodontic referrals were investigated, although the treatment outcomes could not be analyzed because of the short follow-up period. In the present study, 72.8% were treated with only nonsurgical endodontic treatment. This high percentage of nonsurgical endodontic treatment was because of this author's preference. In one study, a higher percentage of endodontists were found to plan an orthograde root canal (re)treatment as a treatment option than that of oral surgeons and general practitioners.14 Since the patients included in this study continue visiting for follow-ups, surgical treatments could increase among this population.
With regard to the treatment procedures, the diagnostic process seems to be important, as 5.8% of the included referrals did not require an endodontic treatment in the present study. Previous studies also indicated that the diagnosis and management of pain is the major reason for referral to an endodontist that may involve teeth other than the ones that were initially diagnosed as problematic.6,15
Conclusions
In the present study, persistent pain was the most frequent reason for an endodontic referral, followed by the presence of gingival swelling and sinus tract, and apical radiolucency. Moreover, pain, apical radiolucency, previous endodontic treatment, and gingival swelling and sinus tract were the major clinical symptoms for the endodontic referrals.

 XML Download
XML Download