

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Vital pulp therapy aims to preserve and maintain the integrity of the pulp that has been compromised by caries, trauma or restorative procedures.1 Indirect pulp treatment (IPT) is one such therapeutic modality and is based on the research of Fusayama et al. who demonstrated that in acute caries, discoloration (affected dentin) preceded the presence of microorganisms (infected dentin).2 The success of IPT depends on adequate reduction of the microbial load, reparative ability of the pulp-dentin complex and placement of a suitable coronal restoration.
Role of remineralizing materials in IPT have been widely investigated, but with conflicting conclusions. Calcium hydroxide (CH) has emerged as the "gold standard" with a success rate of 92 - 97%.3 On the contrary, Eidelman et al. and Pinto et al. have documented similar clinical, radiographic, microbiological and ultra-structural outcome of IPT performed with either CH or inert materials.4,5 This implies that the success of this technique is not dependent on the material applied per se, but on an effective antimicrobial treatment of the deep layers of carious dentin. Another pre-requisite for favorable outcome in IPT is an effective coronal seal. Adequate disinfection is accomplished by physical removal of the infected dentin and entombing the remaining microbes. This creates the conditions for caries arrest and remineralization. However, determining the extent of carious tissue excavation and achieving long-term seal by current restorative materials remain a pitfall. In this context, it is desirable to investigate an effective way of disinfecting the remaining carious dentin.
Photo-activated disinfection (PAD) is an antimicrobial aid that utilizes a photoactive compound (e.g. toluidine blue O, methylene blue) and a light of specific wavelength (600 - 750 nm) to produce oxygen-based free radicals that exterminate the bacteria. PAD is an integral part of the disinfection regimen for root canal therapy due to its dual selectivity, minimal chance of microbial resistance, broad spectrum, instant bacterial killing and ability to target biofilm bacteria. In vitro studies that documented the efficacy of PAD against cariogenic bacteria concluded that it could be an attractive proposition for caries management.6,7 The aim of the present study was to evaluate the role of PAD on the outcome of IPT. The hypothesis was that PAD and CH would result in comparable treatment outcome.
Materials and Methods
Ethical clearance was obtained from the Institute Research Ethics Committee (Ref. No. IESC/T-240/2010). Three study groups were defined on the basis of the material applied, i.e. PAD (Group I), CH (Group II) and PAD followed by CH application (Group III). Subjects between the age group of 18 - 22 years with occlusal carious lesion on molars were included in the study. A detailed clinical history regarding the type, duration, frequency, triggering stimuli and relief from pain was obtained to clinically establish the diagnosis of reversible pulpitis. Subjects with symptoms of irreversible pulpitis/apical periodontitis were excluded. Pre-treatment standardized intraoral periapical and bitewing radiographs were exposed on a size-2 CMOS RVG sensor (Kodak RVG 5100 digital radiography system, Eastman Kodak Company, Rochester, NY, USA) held in a sensor positioning device (RINN XCP-ORA, Dentsply Rinn, Elgin, IL, USA). For all the radiographs, a customized polyvinyl siloxane (Aquasil, Dentsply International Inc., York, PA, USA) bite block was fabricated to register and reproduce the same angulation at subsequent follow-ups. The X-ray unit (ENDO-ACP, Villa sistemi medicali, Milano, Italy) was operated at 70 kV and 7 mA with an exposure time set at 0.12 seconds.
A block randomization method was followed. Sixty teeth were allocated to the pre-defined study groups (n = 20) by an independent statistician through a computer generated random number table. Patient information sheet was provided. The subjects were blinded to the material applied. Written informed consent was obtained.
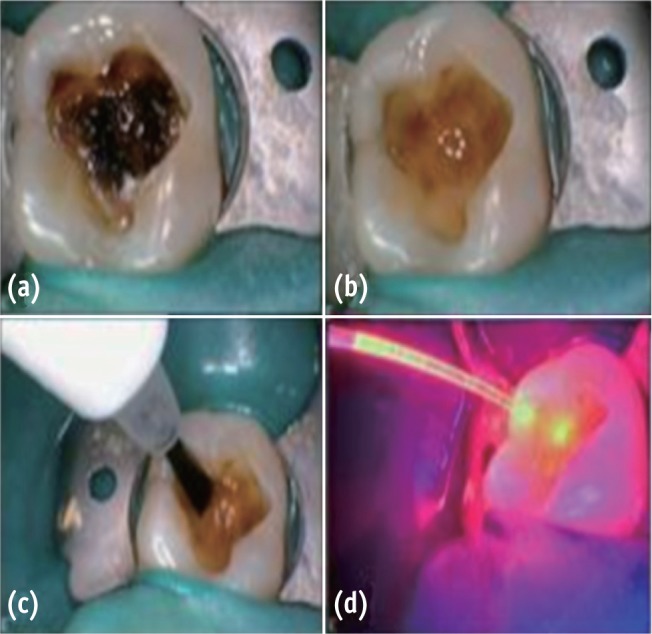
A single operator who was a post graduate student performed all the procedures for IPT on patients under direct supervision of two faculty members. The tooth was anaesthetized (Lox 2%, Lidocaine HCl Injection, Neon Laboratory Ltd., Mumbai, India) and isolated under a rubber dam (Hygenic Dental Dam, Coltène/Whaledent Inc., Cuyahoga Falls, OH, USA). Unsupported enamel and caries from the lesion walls were removed with a sterile #245 tungsten carbide bur (SS White burs Inc., Lakewood, NJ, USA) operated in a high speed air water spray handpiece (Extra Torque 606 C Turbine, KaVo Dental Excellence, Santa Catarina, Brazil). A round tipped probe aided in 'tactile detection' of dentin consistency. In the area deemed "at risk" for pulp exposure, the softened, humid, yellow or light-brown carious dentin that did not offer any resistance to probing was removed with a sterile #6 or #8 carbide bur (SS White burs Inc.) at a low speed handpiece (Ti-Max, NSK, Tochigi, Japan). The darker and harder dentin was preserved.
In group I, PAD solution for caries (0.01 mg/mL tolonium chloride, manufacturer, city, country) was applied with a brush for 60 seconds and irradiated for 60 seconds with PAD system (PAD, Denfotex Light Systems Ltd., Fife, UK). The output was set at 100 mW. The fibre-optic tip was kept at a distance of 2 mm from the carious dentin (Figure 1). The cavity was rinsed with distilled water (Shree Krishna Keshav Laboratory Ltd., Ahmedabad, India) and gently air dried. Cavit G (3M ESPE AG, Seefeld, Germany) was then applied as a sub-base. In group II, CH (Dycal, Dentsply Caulk, Dentsply International Inc., Milford, DE, USA) was applied to the remaining carious dentin without PAD treatment. In group III, PAD application was followed by CH application. The cavities in all three groups were restored with zinc-phosphate base (Mission Dental Inc., Charleston, SC, USA) and silver amalgam (Dispersalloy, Dentsply Int. Inc.; Triple distilled mercury, Chemident Srl, Grosseto, Italy) after application of 2 coats of varnish on the base and cavity walls.
The mid-treatment exclusion criteria included pulp exposure during caries removal and dislodged coronal restoration/tooth fracture. The cases were followed up clinically and radiographically at 45 days, 6 months and 12 months by an independent endodontist who was blinded to the treatment protocol. The criteria used for determining the successful outcome were absence of (1) spontaneous pain and/or sensitivity to percussion, (2) fistula/swelling, (3) pathological mobility, (4) widening of periodontal ligament space, (5) radiolucency at the furcal and/or periapical region, and (6) internal/external dentin resorption.
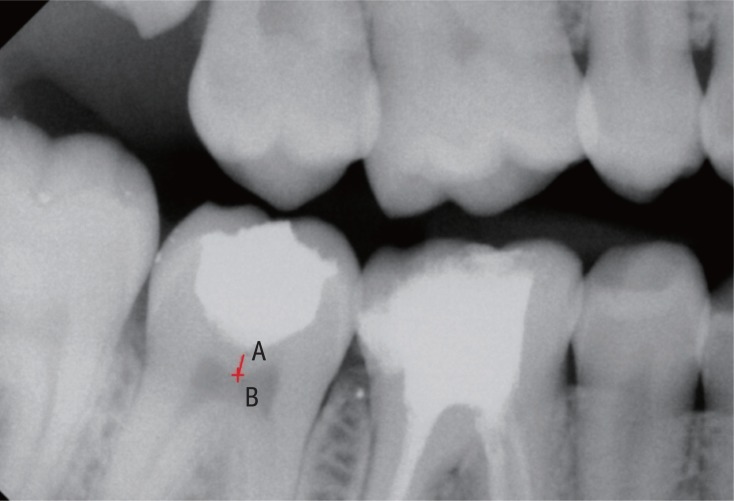
Radiographic evaluation also included measuring of relative density of the remaining dentin using a software available on RVG machine. The 'Intraoral' option in the main menu bar of the Kodak RVG Trophy Imaging Software 6.12.10.0 was used. The 'Tools window' was navigated and 'Densitometric analysis' was clicked. Two defined and repeatable points (i.e. A and B) were identified in the immediate post-treatment and subsequent follow-up bitewing radiographs (Figure 2). 'A' denoted a mark 0.5 mm below the deepest part of the restored cavity and 'B' referred to a mark exactly perpendicular to A on the roof of the pulp chamber. The average grey value along the line joining the two points was noted and correlated with the data obtained on subsequent follow-up. Statistical tests were performed using the Stata 11.0 software (Stata Corp, College Station, TX, USA). The p value was set at 0.05.
Results
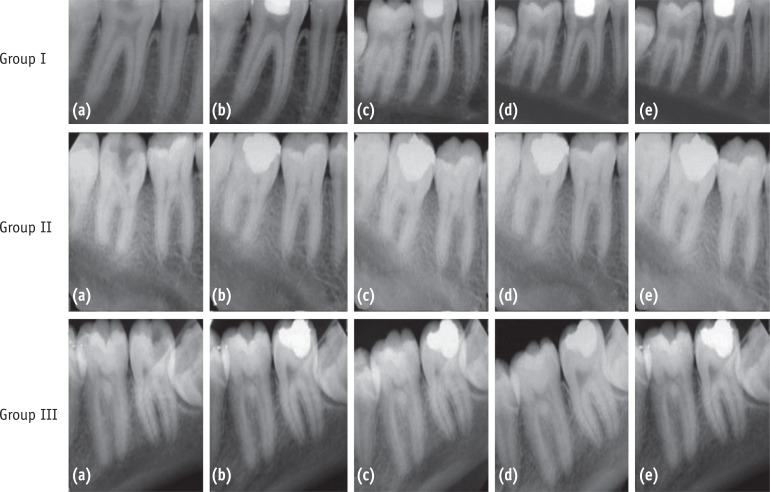
Two teeth had to be excluded due to mid-treatment tooth/restoration fracture. A recall rate of 94.83% was achieved at the end of the study period (n = 55). Fifty four treated teeth showed successful clinical and radiographic outcome at 45 days, 6 months and 12 months (Figure 3). One tooth in Group I reported with signs and symptoms of apical periodontitis and was deemed to be a failure. The three groups were subjected to Fisher's exact test which showed no significant difference (p = 1.000).
The radiographic grey values obtained at the pre-defined follow-up periods in each group were subjected to two-way ANOVA with repeated measures. It revealed that the main effect of groups and the interaction effect (group × time) were not significant with p values of 0.920 and 0.334 respectively. However, the main effect of time was significant (p = 0.0001). At 45 days follow-ups, a significant increase in grey values was observed for group II and III (p < 0.05, Group I: p = 0.16). However, at 6 and 12 months follow-ups, the increase in these values were significant for all the groups (p < 0.05). On inter-group comparison, no significant difference was observed at 45 days, 6 months and 12 months (p > 0.05, Table 1).
Discussion
A carious lesion is radiographically diagnosed to be 'deep' if it penetrates to a depth of two third or more of the entire dentin thickness.8 The IPT protocol for such lesion includes either one visit or two visit (stepwise excavation) procedures. Orhan et al. conducted a study to assess the outcome of one or two visit IPT in 154 primary and permanent teeth.9 No significant difference was observed in terms of success rate. They concluded that either of the approaches could accomplish the desired outcome. The analysis of clinical studies showed high success rates for both one-visit IPT and stepwise excavation.10,11
Equal distribution of the baseline characteristics, a high recall rate and evaluation by an independent endodontist reduced the outcome bias in the present study. The success/failure of IPT were assessed according to the established guidelines.12 In addition, RVG 'densitometric analysis' of the remaining affected dentin was performed. To date, evidence of remineralization of sealed carious dentin has been demonstrated either by micro-hardness analysis or digital subtraction radiography. The former is an invasive technique requiring re-entry into the cavity. The latter faces the difficulty of image registration. Quantitative radiographic assessment is a valuable attribute of digital diagnostic imaging. It can be categorized into geometric parameters (length, area and volume) and densitometric parameters (tissue mass and density). The basis for two-dimensional radiographic densitometric measurement is that the X-ray attenuation increases with the density of the material for a given thickness.13 The radiographic density is a measure of degree of image darkening and is expressed as grey level numeric values (intensity from 0 - 255). Digital radiography achieves this quantitative analysis using a 'Computer Assisted Densitometric Image Analysis' (CADIA) software. It has been used for detecting subtle changes in the mineralization of hard tissues. Kodak RVG Dental Imaging software 6.12.10.0 incorporates a similar tool. This enables the clinician to quantify the density at desirable points, within the plane and defined fields of the radiogram. Di Alberti et al. studied the peri-implant bone density with a RVG densitometric application.11,14 Using a similar method, Radionov et al. evaluated osseo-integration of a replanted tooth in a nine year old patient.15 They concluded that RVG densitometry showed stable values of bone density.
An increase in radiographic grey values of dentin was observed in every group during the follow-up periods. This can be interpreted as remineralization of the porous and softened dentin. However, on inter-group comparison, this change was not significant at any given follow-up time. The results are in agreement with studies by Franzon et al. who questioned the role/need of a remineralizing agent in IPT and concluded that the increase in the density of remaining dentin was due to a mineral gain resulting from the biological response of the pulp.16,17
Photo-dynamic therapy (PDT) or photo-activated disinfection (PAD) was introduced to dentistry by Professor Michael Wilson in 1993.18 Its use has been extended for eradication of oral pathogenic bacteria that cause caries, endodontic infection, periodontitis and peri-implantitis. It is equally effective against oral gram-positive and negative bacteria. It can kill them in planktonic cultures, plaque scrapings, intact bio-films and dentinal carious lesions.19,20,21,22 Williams et al. studied the efficacy of PAD against Streptococcus mutans in carious dentin and collagen matrix; an environment similar to that which would exist within a carious tooth and concluded that it could achieve appreciable kills (99%).23 It is equally effective against other cariogenic microorganisms including Streptococcus sobrinus, Lactobacillus casei and Actinomyces viscosus.6
PAD solution is tolonium chloride which is a pharmaceutical grade of 'toluidine blue O' and belongs to the phenothiazinium class of photo-sensitizer (PS) compounds. The dye is amphiphilic in nature and this is responsible for its effective penetration in both gram positive and negative micro-organisms. It has a dye concentration of 0.01 mg/mL. Above this, formation of dye 'self-aggregates' (dimeric form) occurs and modifies its absorption spectrum.24 Hence the monomeric form was preferred. A laser of 635 nm was utilized as it matches the absorption spectrum of the dye.
The bactericidal action of PAD is a consequence of PS and light interaction. The excited PS molecule interacts with the endogenous oxygen of the target cells via two pathways. The Type I involve electron-transfer reaction resulting in the formation of toxic oxygen species such as superoxide, hydroxyl radicals and hydrogen peroxide. The Type II process entails energy transfer from the PS triplet state to ground state molecular oxygen, resulting in production of excited singlet oxygen (1O2). These reactive species induces DNA and cytoplasmic membrane damage leading to bacterial cell death.18
It is desirable to have a short exposure time for clinical convenience. Williams et al. demonstrated that energy dose of 1.8 Joules or more killed 100% of the carious bacteria present.7 This can be adjusted and calculated by multiplying the exposure time (second) and the laser output power (mW). An energy dose of 6 Joules (60 seconds × 100 mW, 1 mW = 0.001 J/sec) was utilized in this study. This was sufficient for a profound antibacterial action and safe for pulp vitality.25
The proposed hypothesis was sustained based on the success of IPT achieved in all groups. The results suggest that PAD and CH both have equal disinfection efficacy in the treatment of deep carious dentin. PAD probably provided an effective and convenient method for reducing the microbial load of the remaining carious dentin. Clinically, this would make it less critical to distinguish between infected and affected dentin. 'Favorable conditions' for healing of the pulp-dentin complex can be achieved without the placement of a remineralizing material.
The present pilot clinical work was based on the premise that PAD is a highly effective antibacterial treatment modality. However, further in vivo microbiological investigations need to be conducted to establish the efficacy of PAD for disinfection of deeper layers of carious dentin. Usefulness of 'RVG Densitometry' as a viable tool for measuring relative density of dentin needs further investigation as well. To positively substantiate the results of the present study and establish PAD in the treatment protocol of IPT, longitudinal studies with larger sample size would need to be undertaken.
Conclusions
PAD and CH both have equal disinfection efficacy in the treatment of deep carious dentin. PAD alone is as effective for treatment of deep carious lesion as CH and hence can be used as an alternative to CH. They can be used independently in IPT, since combining both does not offer any additional therapeutic benefits.

 XML Download
XML Download