

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Dental caries is a dynamic disease, governed by multiple contributing factors under individual circumstances. in situ models are useful as surrogate models of large-scaled, randomized controlled clinical trials (RCT) in caries studies.1 To achieve a high level of clinical relevance, in situ models need to simulate uncontrolled intraoral conditions, incorporating highly-controlled experimental parameters.2 Since multiple combinations of natural and experimental variables are included in in situ models, the study designs are complicated under various limitations. Additional factors are related to the power of analysis, such as sample sizes and sample allocation methods.1,3 Compared to RCT, in situ models require a relatively small group of participants. However, a high degree of compliance with precisely-defined protocols is crucial. Designing optimized in situ models is a demanding step for researchers, who often refer to published literature with a similar topic and interest to their own. However, there are numerous protocols involving various parameters in in situ set-ups, resulting in reader confusion. For study design and evidence seeking, there is uncertainty in how to correlate dissimilar outcomes among each other which were produced from different experimental conditions.
The aim of this study was to analyze the pre-existing protocols of in situ caries models and to provide an informative guideline for study planning. We evaluated published articles, focusing on materials and methods. We organized parameters implemented in each in situ model to validate its methodological aspect. Our reasoning was that there would be some conditions and factors frequently used in current in situ caries models and that would be largely applicable to future studies. Furthermore, in situ studies can be performed in closely-related standardized manners. The data interpretation and application can be enhanced to increase our knowledge in the area of cariology.
Materials and methods
A search was performed using the online PubMed database with the following keywords, (in situ) AND (enamel OR dentin OR caries OR demineralization OR remineralization OR erosion). The initial search identified 265 titles and abstracts on March 25, 2013. Original full articles written in English were included and screened by two independent investigators (Figure 1). The primary screening excluded twenty articles because (1) the studies were not performed on in situ models (n = 13) and (2) only abstracts were available (n = 7). Secondary screening included articles within the scope of cariology, excluding 54 articles in the following areas, (1) medical fields (ophthalmology, urology, or others, n = 9), (2) dental fields other than cariology (prosthodontics or periodontology, n = 15), (3) tooth whitening focused only on color changes (n = 10), (4) dental materials without teeth involved (n = 9), (5) hypersensitivity treatment involving dentinal tubule occlusion (n = 7), and (6) biofilm evaluation without teeth involved (n = 4). A total of 191 articles published in 35 journals were reviewed for analysis (Table 1). One investigator produced a data formulation sheet, while the other investigator independently filled the sheet with information from ten randomly selected articles.4 Assessment and agreement were reached between the two investigators during the preliminary procedure. The extracted data from the included articles were organized according to the following factors, (1) publication types: publication years and main topics (demineralization, remineralization, erosion, and others), (2) study population: participant background, inclusion criteria, sample sizes, sample size justification, and sample allocation methods, (3) specimens and appliances: tooth types, specimen numbers, intraoral appliance types, and sterilization methods, and (4) other protocols: appliance-wearing periods, wash-out periods, supervising methods, experimental interventions, and outcome measures.
Frequencies and percentages of the articles were displayed according to the publication types, characteristics of the population, factors on the specimens and appliances, and other protocol types. Pearson's chi-square test was used to assess statistical significance at a type one error rate of 0.05. The statistical software SPSS 12.0 (SPSS Inc., Chicago, IL, USA) was used in the analysis procedure.
Results
Publication types
The journals with in situ studies published are listed in Table 1. Caries Research was the journal with the highest number of articles of published in situ caries studies (n = 63, 33.0%). The yearly distribution of publications of in situ caries studies according to their main topics is shown in Figure 2.
Study population
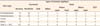
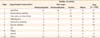
The most frequently applied inclusion criterion was normal salivary function of the participants (87 articles, Table 2). The next most common criteria were the general health of the participants (83 articles), followed by the dental status of the participants (74 articles). The selected numbers of participants for each study ranged from 10 to 14 in 96 studies (50.3%, Table 3). Larger groups of participants (≥ 25) were included in 28 studies (14.7%). Sample size justification was stated in 42 articles (22.0%). There was no significant correlation between the proof of sample size justification and the numbers of participants or specimens. Sample allocation was randomized in 76 studies (40.0%), and cross-over was done in 145 studies (76.0%, Table 4). While significantly smaller percentages of randomized trials were performed in studies with the topic of demineralization (26.8%), significantly larger percentages of those were done in studies with the topics of remineralization (49.3%), erosion (42.3%), and other (50%, p < 0.05). The proportions of cross-over designs were similar across the main topics (p > 0.05). Double- or triple- blinded experiments were performed more frequently in the remineralization studies compared to studies with other topics (p < 0.05). The vast majority of studies (83.8%) did not state who comprised the study participants. Participants were staff or students from dental schools in 22 studies (11.5%) and dental patients in six studies (3.1%), while public recruiting occurred in two studies (data not shown).
Specimens and appliances
The numbers of tooth specimens embedded in a single appliance were mostly 2 to 4 (64.9%, Table 3). Removable types of intraoral appliances were applied in 172 studies (90.0%, Table 5). Among the 18 studies that used fixed appliances, lower molars were used in nine. A total of 128 in situ studies used human teeth (67.0%), particularly third molars (68 studies, 35.6%, Table 6). Bovine incisors were used in 63 studies (33.0%). Storage of teeth in formaldehyde was the most common method for sterilization (24.0%), followed by thymol (16.2%) and ethylene oxide (12.7%). Sterilization methods were not significantly different between human and bovine teeth.
Other protocols
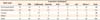
The period of wearing appliances ranged from four to eight weeks in 55 studies (28.8%, Table 7). The total period of a study including a wash-out period was from four to eight weeks in 60 studies (31.4%). A wash-out period was applied in 110 studies (57.6%), usually for less than two weeks (68 studies). A total study period including a wash-out period was longer than four weeks in 127 studies (66.5%). The most frequently applied experimental intervention was dentifrice (67 studies), followed by mouthrinse (27 studies), drinks (22 studies), and chewing gum (16 studies, Table 8).
Additional descriptions were given on supervising methods for participant's compliance such as, (1) records or diaries (24 studies), (2) questionnaires or letters (15 studies), (3) check-up of the amount of materials used (toothpaste, mouthrinse, or others, five studies), and (4) measurements of salivary fluoride (two studies). No description was given on the supervising procedures in 153 studies.
For an assessment of the experimental outcomes, a surface or cross-sectional microhardness test was most commonly used (74 studies), followed by transmitted microradiography (TMR, 65 studies, Table 9). TMR was the most commonly chosen technique in the remineralization studies (42.1%), and profilometry was mostly used in the erosion studies (54.4%).
Discussion
The application of in situ models in a caries study is an interim method between clinical trials and laboratory experiments, which provides many advantages. RCT usually offers the highest level of evidence, but there are some parameters that need to be optimized, but are not easily applicable. Moreover, the prevalence of dental caries has decreased worldwide in the past few decades. In RCT, a very large number of subjects are required to be studied for a long period of time in order to determine the effect of a certain intervention. Alternatively, in situ studies can be conducted with a small group of participants in a much shorter period of time, imposing many controllable variables.2 It is essential for in situ studies to construct a protocol appropriate for a specific clinical question in a practical way. Researchers usually rely on references chosen from their own perspectives. Often, various protocols are produced by their value judgments which are personal and subjective preferences under individual circumstances.5,6,7 We thought that it was necessary to collect and evaluate preexisting protocols to overcome the methodological heterogeneity in in situ caries models. This evaluation may not help academic or clinical experts perform caries studies specifically for their elaborated hypotheses. More likely, the information would provide guiding information for young researchers or clinicians who want to solve their academic questions in a more clinically relevant way than through laboratory experiments.
We categorized the included articles according to the main topic of the articles. We selected three major issues among the published articles (demineralization, remineralization, and erosion), and 95% of the articles in the review fell to these three topics. The remineralization and erosion topics seemed to have gained interest during the past decade (Figure 2). The relationships between the research topics and their experimental protocols were not remarkable even though the outcome measurement of the studies differed in relation to their topics. An extent of remineralization was mainly assessed using TMR, which showed the cross-sectional topography of the tooth specimens with changes in the demineralized subsurface areas. In the erosion study, profilometry and microhardness tests were exclusively applied to investigate the superficial characteristics.
One of the main barriers in carrying out in situ studies may be recruiting the appropriate number of participants. Only a few articles mentioned the source of the participants. The study groups mostly consisted of a dental-related population that, from many perspectives, was not representative of the general public. This reflected difficulties in collecting volunteers who are willing to follow intricate instructions and tolerate possible discomforts. Even with recruiting, the ability to maintain the compliance of the participants throughout an entire trial is another concern. Only a limited number of studies mentioned this issue, but did not go into details. The number of participants required is also important for study preparation. Sample size calculation plays a critical role in detecting clinically important differences in trials.8 Although dissimilar outcome measurements were chosen by each individual study, the number of participants mostly ranged from 10 to 14. Most articles did not disclose sample size justification. The numbers of tooth specimens embedded in a single appliance were 2 to 4 in 65% of the studies, which seemed to make specimen preparation technically feasible. The next step may be to determine how to fabricate intraoral appliances. The appliances should be appropriate for participants' safety and comfort with all specimens securely fixed. Regardless of the research topics, the most common prototype was a removable maxillary appliance. Conventional holly-typed metal appliances tended to be replaced into acrylic palatal appliances.9 With an increasing number of in situ bleaching studies, soft bleaching trays were also modified with palatal extensions.10 The sterilization method of the tooth specimens is another issue, since the biological tissues obtained from other donors were attached to the intraoral appliances. In addition, it would produce a mental barrier for some appliance-wearers. Some institutional review boards only allowed for the participants to wear the appliance including tooth slabs provided from the same individual, which made it more challenging to recruit participants. The sterilization method that was primarily used was immersion of teeth in sterilizing media such as formaldehyde or thymol. Ethylene oxide gas and gamma radiation were also used, but those frequencies were low due to the additional costs and facilities required. It may be more important to eliminate the soft tissue from the tooth specimens versus using a specific disinfectant.11 However, only a few articles had mentioned removing pulpal tissue and periodontal ligament during specimen preparation. The risk of prion transmission through dental tissue had not been clearly established and was only a potential concern.11 Based on our analysis, the sterilization methods were not significantly different whether human or bovine teeth were used. The period of wearing appliance was also crucial to obtain participants' consent. A large proportion of studies introduced a wash-out period, providing baseline observations before entering a trial, or eliminating any effects from predisposed interventions in crossover studies. Wash-out periods extended the total study periods by one to four weeks, and the whole study periods were longer than four weeks in 67% of the studies.
This study only analyzed the methodological aspects from the reviewed articles. It is different from conventional systematic reviews or meta-analyses which summarize the results of the included studies. However, according to the current terminology used for a systematic review, it was denoted as a review of a clearly formulated question using systematic and explicit methods by collecting and analyzing data from publications.12 Our research question was whether any parameters or conditions had been commonly included in the previous protocols of the in situ caries studies. Even on our attempts of gathering comprehensive information, data extraction from the reviewed articles may be incomplete, leaving some other variables without consideration. A future systematic review should include as many relevant variables as possible to constitute the integration of an in situ model. With accumulation of data produced from standardized protocols, an effect size from each variable can be easily calculated for statistical analyses. A complete form of meta-analysis can then be achieved.








 XML Download
XML Download