

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A thorough knowledge of the anatomy of root canal system is required to improve the success rate of endodontic treatment.1-4 Because the root canal system is complex, canals may branch, divide, and rejoin taking various pathways to the apex. In clinical situation, clinicians usually depend on two-dimensional radiograph for understanding the anatomy of root canal system. The early recognition of these configurations facilitates cleaning, shaping, and obturation of the root canal system. Unfortunately, two-dimensional radiographic images do not reveal all anatomic characteristics.5,6
Furthermore, the apical foramen often does not represent a round shape.7 Many root canals represent an oval or flat apical foramen that makes measuring the diameter of root canals difficult.8-10 With regard to obturation, some studies verified that many of the canal surfaces (especially in the apical region) are not touched during canal preparation because of the oval or irregular configuration.11-13 These untouched canal surfaces may account for the failure of endodontic treatment.
Weine categorized the root canal systems in single root into four basic types: Type I, single canal from the pulp chamber to the apex; Type II, two separate canals leaving the chamber but merging short of the apex to form only one canal; Type III, two separate canals leaving the chamber and exiting the root in separate apical foramina; Type IV, one canal leaving the pulp chamber but dividing short of the apex into two separate and distinct canal with separate apical foramina.14 Vertucci et al. had reported the anatomy of Type II root canal systems.15 The complexity of Type II root canal systems prevents these canals from being cleaned, shaped, and obturated effectively during root canal therapy. Once recognized, the type II root canal systems provide challenges with respect to debridement and obturation. In point of debridement, Jeong et al. investigated the sizes of master apical file by instrumentation in type II root canal systems.16
The aim of this study was to investigate the relationship between the apical foramen morphology and the length of the merged canal at the apex in type II root canal systems.
Materials and methods
1. Selection and preparation of teeth
The teeth were collected from a general dental practice and had been extracted for pulpal, periodontal, and orthodontic reasons. This study included intact extracted maxillary and mandibular human premolars (n = 20) with fully formed roots without any visible signs of external resorption. None of these teeth had prior root canal treatment. The teeth were manually cleaned from the calculus and periodontal tissues. The teeth were stored in a 0.1% chlorhexidine solution. Preoperative radiographs were taken to estimate the root canal type. And the teeth with Type II root canal systems were classified. The root segments were obtained by removing the crown 1 mm beneath the cementum-enamel junction (CEJ) using rotary diamond disk. The root canals were negotiated with a size 10 K hand file to avoid modifying the canal's apical anatomy and irrigated with 5.25% sodium hypochlorite.
2. Measurement
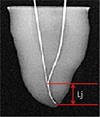
The reference length of the root canal was measured as follows. First, a size 10 K hand file was inserted into the root canal until the file tip was visible at the apical foramen. Another 10 K hand file was inserted into the root canal until the file tip was joined with existing file. The two 10 K hand files joined at the point. The distance between the file tip and merged point of joining two canals was defined as Lj. And Lj was measured using ImageJ program (1.44p, National Institutes of Health, Bethesda, MD, USA). Postoperative radiographs were taken to estimate Lj (Figure 1).
3. Evaluation
The specimens were embedded in epoxy resin. After the epoxy resin had set, the roots were carefully sectioned at 1 mm from the apex by slow-speed water-cooled diamond saw (Isomet, Buehler Ltd., Lake Bluff, IL, USA) positioned perpendicularly to the root canal and prepared for microscopic analysis. Each cross section was prepared with ethylenediaminetetraacetic acid (EDTA) irrigant (PREP EDTA Gel, Vision, Seoul, Korea) for 5 minutes, then rinsed with saline and dried. Afterwards, each cross section was stained with methylene blue to highlight the contours of the root canal, then rinsed with saline and dried. All cross sections were examined under the microscope (BX60MF, Olympus Optical Co. Ltd., Japan) at ×50 magnification and photographed to estimate the shape of the apical foramen. The longest and the shortest diameter of apical foramen was measured using ImageJ program (1.44p, National Institutes of Health). Criteria of the apical foramen shapes were as follows. A root canal which two diameters were equal was categorized as round shape. Likewise, a root canal that one diameter is longer than another one by more than the radius was oval shape. Lastly, one with the diameter 2 times longer than that of another was flat shape.
4. Statistical analysis
For each cross section, the proportion (P) between the longest (Dl) and the shortest diameter (Ds) was related to Lj. Correlation coefficient was calculated to identify the link between Lj and the apical foramen shape by Pearson's correlation. All data were summarized with means, maximum, minimum, standard deviation (SD) and analyzed correlation between Lj and the apical foramen shape using the software SPSS version 17.0 (SPSS Inc, Chicago, IL, USA).
Results
The distance between the file tip and merging point of two joining canals (Lj), the longest diameter (Dl), the shortest diameter (Ds), the proportion between Dl and Ds (P) and the apical foramen shape (AFS) was shown in the Table 1. The apical foramen shape from this study was indentified as oval or flat (Figure 2). The average of Lj was 3.74 mm (Max, 9.30 mm; Min, 0.00 mm). The average of P, estimated by dividing the shortest diameter into longest diameter of the apical foramen, was 3.64 (Max, 24.93; Min, 1.16) (Table 2).
The shape of the apical foramen was recognized depending on the P. When the P was smaller than 2.00, the apical foramen shape was close to oval. When the P was larger than 2.00, the apical foramen shape was close to flat. We hypothesized that if Lj is longer, P is close to 1.00. To prove this hypothesis, we calculated a correlation coefficient (Pearson's correlation). Table 3 showed the correlation coefficient of two variables. Since it was a negative figure (- 0.463) and statistically significant (p < 0.05), there was inverse correlation between Lj and P. Therefore, the hypothesis was reasonable. Therefore, in condition of the type II root canal system, the longer Lj was, the smaller P became, and the shorter Lj was, the larger P became. Namely, the longer Lj was, the more oval contour of apical foramen became. Likewise, the shorter Lj was, the more flat contour of apical foramen became.
Discussion
Successful endodontic treatments require the knowledge of the apical foramen shape and size. It is essential to determine the size of apical preparation. The observations of the apical foramen shape in the present study are in disagreement with previous findings. Martos et al. found that the most frequent root apex morphology and apical foramen in the maxillary and mandibular teeth was the round shape, and the oval shape was second.10 But, major findings from these samples included demonstration of oval and flat shape of the apical foramen as same proportion (each 50%). In this study, only Type II root canal systems were examined, and we observed the oval and flat apical foramen shape. In this point of view, the mechanical canal enlargement might be insufficient for cleaning the type II root canal systems. Therefore, irrigations with chemical solution such as NaOCl, CHX, and EDTA were also very important for disinfection of the root canal.17,18
There is little controversy about the size of the apical preparation, and it is significant when considering the best possible debridement of infected root canals.19,20 To determine the size of apical preparation in clinical situation, clinicians might use the two-dimensional radiographic image. This procedure reflects the clinical situation. Clinician might measure the distance between file tip and the merged point of joining two canals. Jou et al. suggested constant criteria to estimate the apical foramen shape.21 As it becomes shorter, the flatter the apical foramen become. Therefore, the size of the apical preparation should be considered for mechanical debridement of infected root canals.
Although the present study clearly showed the negative correlation between Lj and P, it had several limitations, which need to be mentioned. The methodology used to calculate the morphology, the different ages of specimens, and the small number of groups investigated could cause slight variation.22 Some specimens had curved root canals. Thus, it was difficult to measure the length of specimens. In addition, we had used the two-dimensional radiographic image to measure the file length. Unfortunately, the two-dimensional radiographic images did not reveal all anatomic characteristics. The different ages of specimens probably could interfere with the results of the anatomic evaluation. The reason is that the constant remodeling of the root apex occurred through cementum apposition and resorption.23 There are few articles about the length of merged canal in type II root canal system. In this study, the average of Lj was 3.74 mm (Max, 9.30 mm; Min, 0.00 mm). Park et al. mentioned the length of merged canal in first molar mesiobuccal root of the maxilla, but the data is a little different from the findings of this study.24 This difference may be caused by the type of teeth.
In this study, oval and flat apical foramen shapes were observed. It was difficult to measure the diameter of apical foramen in these types. And it was impossible to remove the debris with only mechanical instrumentation. Therefore, it needs to be considered that use of endodontic instruments do not touch the certain surface of the root canal system. Also, a better method of cleansing and disinfecting the root canal should be researched. The observations made here will provide a more precise understanding of the type II root canal system. In the next study, we need to classify the teeth according to a type. Correlation between the file length (Lj) and the proportion of diameter in each type of the teeth needs to be investigated in the future.
Conclusions
There was an inverse correlation between Lj and P. As the distance between the file tip and merging point of two joining canals gets longer, the apical foramen becomes more oval shaped. Likewise, as it gets shorter, the apical foramen becomes more flat shaped. Therefore, clinician should consider the shape and size of apical foramen according to the length of merged canal during root canal instrumentation in type II root canal system.



 XML Download
XML Download