

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The ultimate goal of root canal preparation is to clean and shape the root canal system while maintaining the original configuration. Over the years, many nickel-titanium (Ni-Ti) instruments have been developed to improve root canal preparation. They are available in various designs that differ in tip and taper design, rake angles, helical angles, pitch, and presence of radial lands.
Two brands of Ni-Ti instruments adopting the single-file system were recently introduced to the market and advocated the reciprocation concept: Wave·One (Dentsply-Maillefer, Ballaigues, Switzerland) and Reciproc (VDW GmbH, Munich, Germany). These files are made of a special Ni-Ti alloy called M-wire that is created by an innovative thermal-treatment process.1 This procedure has been developed using superelastic Ni-Ti wire blanks that contain substantial stable martensite under clinical conditions. The benefits of M-wire are increased flexibility of the instruments and resistance to cyclic fatigue.2
These files have a different mechanism of instrumentation compared to other previously developed files. The system is designed to be used with a dedicated reciprocating motion. The values of clockwise and counterclockwise rotations are different. A large rotating angle in the cutting direction (counter-clockwise) determines that the instrument advances in the canal and engages dentin to cut it, whereas a smaller angle in the opposite direction (clockwise) allows the file to be immediately disengaged and safely progress along the canal path, while reducing the screwing effect and file separation.3
In clinical practice, these Ni-Ti instruments carry a risk of fracture mainly because of flexural and torsional stresses.2,4,5 This risk may be reduced by performing coronal enlargement and preflaring manually to create a glide-path before using Ni-Ti instruments.3,6-8 However, the manufacturer of Reciproc instruments does not strictly recommend creating a glide-path when using the reciprocating instrumentation. In contrast, a glide-path of at least size 10 is recommended in the manufacturer's instructions for the use of Wave·One instruments. The glide-path is a smooth radicular tunnel from the canal orifice to the physiologic terminus.9 Blum and colleagues suggested creating a glide-path using small flexible stainless steel hand files to create or verify that within any portion of a root canal there is sufficient space for rotary instruments to follow.10 In general, a glide-path was prepared using #15 K-file to ensure sufficient space for the file to work and to avoid the risk of locking.
There are only limited studies available concerning the centering ability and preparation time of these recently introduced instruments by using reciprocating motion. Therefore, a comparison of these single-file systems with or without glide-path is necessary to assess the properties of these new files. The aim of this study was to evaluate the shaping ability of the newly marketed single-file instruments in terms of maintaining the original root canal configuration and curvature, with or without a glide-path.
Materials and Methods
Root canal instrumentation
Forty simulated curved root canals in clear resin blocks (Dentsply-Maillefer) were used for this study. An apical foramen size of 0.1 mm was confirmed, and each canal had a mean canal length of 17 mm. Each simulated canal was colored with red ink injected using a syringe. The blocks were divided into 4 groups according to the instruments used: Group 1, no glide-path / Wave·One (NW); Group 2, no glide-path / Reciproc (NR); Group 3, #15 K-file / Wave·One (KW); Group 4, #15 K-file / Reciproc (KR). For Groups 1 and 2, a glide-path was not established. For Groups 3 and 4, a #15 hand K-file was used after a #10 hand K-file had been used.
The Reciproc R25 instrument and Wave·One Primary file, both of which had a tip size of 0.25 mm and a 08 taper in the apical 3 mm, were selected. The files were operated with the Silver Reciproc motor (VDW GmbH) with their respective recommended settings: Reciproc with the "RECIPROC ALL" mode and Wave·One with the "WAVEONE ALL" mode. Reciproc and Wave·One were used in a reciprocating, slow in-and-out pecking motions. The flutes of the instruments were cleaned using gauze soaked with 70% ethyl alcohol after 3 in-and-out movements. Each instrument was discarded after use in 2 canals.
Assessment of canal preparation
Pre- and post-instrumentation images were scanned and recorded. The images were superimposed using a computer software program (Photoshop 7.0, Adobe, San Jose, CA, USA). The ability of the instruments to remain centered in the canal was determined by calculating a centering ratio using perpendicular lines made by the canal axes at 1, 2, 3, 5, and 7 mm (Figure 1a). The centering ratio was calculated using the formula (X1-X2)/Y, where X1 represents the maximum extent of canal movement in one direction, X2 is the movement in the opposite direction, and Y is the diameter of the final canal preparation (Figure 1b). The data were analyzed using the SPSS program (version 10.0, SPSS GmbH, Munich, Germany). Changes in canal curvature and centering ratios at the 5 measuring points were statistically analyzed using one-way analysis of variance (ANOVA; α = 0.05) followed by Tukey's test.
Topographic analysis using scanning electron microscopy (SEM)
The cyclic fatigue stress was loaded to examine the cross-sectional shape of fractured surface. In brief, an artificial canal block made of tempered steel with 0.6 mm apical diameter, 6.06 mm radius, and 45° angle of curvature, measured according to the method of Schneider, was incorporated into the blocks.11 A continuous up-and-down (4 mm in each direction at 0.5 second) pecking movement was incorporated to simulate the pecking motion in a real clinical situation. The files were operated in the VDW.SILVER motor (VDW) with each recommended setting: Reciproc files with the "RECIPROC ALL" mode and WaveOne with the "WAVEONE ALL" mode. Then, the broken fragments were evaluated under the SEM (S-4800 II; Hitachi High Technologies, Pleasanton, CA, USA) for topographic features of the fracture surfaces at various magnifications (180 - 200 times).
Results
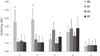
As shown in Figure 2, at the 1 and 2 mm levels, the mean centering ratio was statistically significantly higher in Group 1 (p < 0.05). The centering ratio at the 3, 5, and 7 mm levels showed no statistically significant difference (p > 0.05).
The two reciprocating file systems used in this study have different cross sections, S-shaped and concave triangular shape for Reciproc R25, Wave·One, respectively (Figure 3).
Discussion
Recently, new systems that use reciprocating motion were introduced to the market, claiming to be able to shape root canals using a single file. These file systems make canal shaping simpler and faster. Reciprocation motion was proposed to increase the canal centering ability as well as to reduce the risk of root canal deformity.12-14 However, there have been little information about the centering ability of these files systems in curved root canals.
To assess the instrumentation of curved canals, clear resin blocks were used in this study. These were chosen because the shape, size, taper, and curvature of the experimental canals were standardized. The credibility of resin blocks as an ideal experimental model for the analysis of endodontic preparation and preparation techniques has been validated by Weine et al. and Dummer et al.15,16 However, there are limitations with the model, such as the different hardness between resin and dentin, and care should be exercised in the extrapolation of the present results to the use of these instruments in the clinical setting. A major drawback of using rotary instruments in resin blocks is the heat generated, which might soften the resin material and lead to binding of the cutting blade and separation of the instrument.17-19 Nevertheless, the use of simulated canals in resin blocks allows for the standardization of the research method and to exclude parameters that could influence the preparation outcome.
Proper shaping of the canal to create a continuously tapered funnel form is one of the most important objectives for root canal preparation. It facilitates irrigation and obturation of root canals.20 However, during preparation, some root canal aberrations are created, such as transportation, elbow, and apical zip. It has been shown that root canal instrumentation leads to changes in the working length by straightening of the curved canal during the course of the treatment.21 These aberrant results of root canal shaping make it difficult for clinicians to remove the infected tissue and properly obturate the root canal.22
The centering ratio can define the ability of instruments to remain centered in shaped canals. According to the formula, the centering ratio approaches zero as X1 and X2 become closer to the center. The lower the scores, the better are the instruments centered in the canal. In this study, the results of the assessment of the centering ratio in the 4 groups at 1 and 2 mm levels indicated that the ability of the instruments to remain centered in prepared canals was significantly lower in the no glide-path / Wave·One group. The tip size (diameter at D0) of Reciproc R25 and Wave·One primary were the same with each other. The two reciprocating file systems are made of the same alloy (M-wire) but have different cross sections, S-shaped and concave triangular shape for Reciproc R25 and Wave·One, respectively (Figure 3). The larger canal abberation achieved for the no glide-path/Wave·One group at 1 and 2 mm level might be due to the larger core diameter and greater number of spiraling flutes of Wave·One. The larger core diameter and greater number of spiraling flutes of the Wave·One instrument increases the stiffness of the tip, which results in more canal abberation.
Conclusions
Conclusively, the ability of the instruments to remain centered in the prepared canals at the 1 and 2 mm levels was significantly lower in Group 1 (no glide-path / Wave·One). However, the centering ratio at the 5 and 7 mm levels were not significantly different. The current study shows that both of the instrumentation systems possess an adequate centering ability. However, Wave·One should be used following establishment of a glide-path larger than #15.


 XML Download
XML Download