

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Tooth avulsion is a serious traumatic injury ranging from 0.3 to 5% of all dental injuries in the permanent dentition.1 Tooth loss after the injury can cause a significant esthetic problem and psychological trauma to the patient.2,3 Indeed, the most frequently affected teeth are the maxillary central incisors, which are esthetically and psychologically critical in growing young patients.2,3 As a treatment modality, tooth replantation has been suggested for avulsed teeth. However, replanted teeth succumb to root resorption with an occurrence of 50 to 76%, and even if managed properly, still lead to tooth loss in many clinically cases.4-6 Irreversible damage on surrounding periodontal apparatus during avulsion is likely to be considered a main etiology of root resorption and tooth loss.7
Due to the great risk of tooth loss after tooth avulsion, a variety of adjunctive treatments have been proposed to prevent and delay root resorption, thereby increasing the survival of replanted teeth. Fluorides, steroids, sodium alendronate, and enamel matrix derivatives (EMD) have been used as therapeutic agents for this purpose.8-11 Among them, EMD has been widely used as a topical agent in replantation of avulsed teeth.11,12 Emdogain (BIORA AB, Malmo, Sweden), a commercialized EMD product, was developed for the regeneration of periodontial tissues. Emdogain contains an enamel matrix protein extracted from developing porcine embryonic enamel in a sterilized aqueous solution of propylene glycol alginate.13 It was shown that enamel matrix proteins were incorporated during the development of acellular cementum on the root surface, where Sharpey's fibers could attach.14,15 Therefore, it has been suggested that the periodontal attachment may be stimulated if a root surface is treated with EMD.
The effect of EMD on periodontal healing and root resorption after tooth replantation has been investigated in many preclinical and clinical studies. However, there are controversies with regard to the regenerative role of EMD in replanted teeth. Indeed, EMD was shown to promote periodontal healing during replantation in some studies, whereas in other studies, EMD did not prevent root resorption.11,16-29 Wiegand and Attin in their systematic review attempted to statistically analyze the impact of EMD on healing of replanted teeth.30 However, due to lack of randomized controlled trials and clinical controlled trials, no conclusion could be drawn in the review.
In this systematic review, we hypothesized that the presence of periodontal ligament (PDL) on root surface was critical for normal periodontal healing when EMD was applied before tooth replantation. The purpose of this study was to investigate the effect of EMD on healing of replanted teeth in preclinical animal models and answer the following research question in the Population, Intervention, Comparison, Outcome (PICO) format: "For animals with replanted avulsed teeth (population), will EMD treatment (intervention) increase normal periodontal healing or decrease root resorption (outcome) compared to no EMD treatment (comparison)?"
Materials and methods
Literature search and selection criteria
The following electronic databases were searched for articles published up to October 2012: MEDLINE, PubMed, EMBASE, Cochrane Library, Web of Knowledge and Scopus. The search strategy was as follows: ('Emdogain' OR 'enamel matrix protein' OR 'enamel matrix derivative') AND ('avulsion' OR 'transplantion' OR 'autotransplantation' OR 'replantation'). Inclusion criteria consisted of controlled animal studies in which EMD was applied in transplanted or replanted teeth. Outcome data of the controlled animal studies were determined by histology. Exclusion criteria consisted of studies without controls, studies with only radiographic data presented, review papers as well as studies that did not meet the inclusion criteria.
Outcome measures and data extraction
Data were extracted according to the following outcome measures: normal periodontal healing, surface root resorption, inflammatory root resorption and replacement resorption. Two reviewers (SK, SR) independently extracted data on the basis of these outcome categories. Any discrepancies were resolved by collective discussion. If data were missing, the authors of identified controlled studies were contacted for further information.
Quality assessment
The assessment of the quality of included studies was performed independently and in duplicate by the reviewers (SK, SR). The criteria for assessing the quality were modified from the guidelines proposed in the Cochrane Handbook.31 Included studies were assessed by the consideration of the following criteria: the method of randomization (exclusively for randomized controlled trials), allocation concealment (exclusively for randomized controlled trials), masking of examiners for outcome assessment, completeness of follow-up period, and balanced experimental groups.
Assessment of heterogeneity
The heterogeneity of included studies was evaluated with the following variables: animal species, follow-up period, extraoral time, endodontic treatment, and the presence of PDL and use of ethylenediamine tetraacetic acid (EDTA) prior to EMD application.
Statistical analysis
The subgroups of individual studies were identified based on their study designs for statistical analysis. For the studies that had subgroups with similar study designs and outcome measures, a meta-analysis was performed to calculate the effect size of the studies and 95% confidence interval. Statistical analysis was performed using the software Comprehensive Meta Analysis version 2 (Biostat, NJ, USA).
Results
Quality assessment
One study was a randomized controlled trial,29 but the other studies were controlled trials.17,24,25,26,32 The method of randomization, allocation concealment and masking of examiners for outcome assessment was unclear in this randomized controlled trial, and masking of examiners for outcome assessment was also unclear in the controlled trials. All included studies showed completeness of follow-up period except one study, in which some samples were lost during the extraction and histological processing.17 The number of samples in experimental groups within individual studies was well balanced in all included studies.
Assessment of heterogeneity
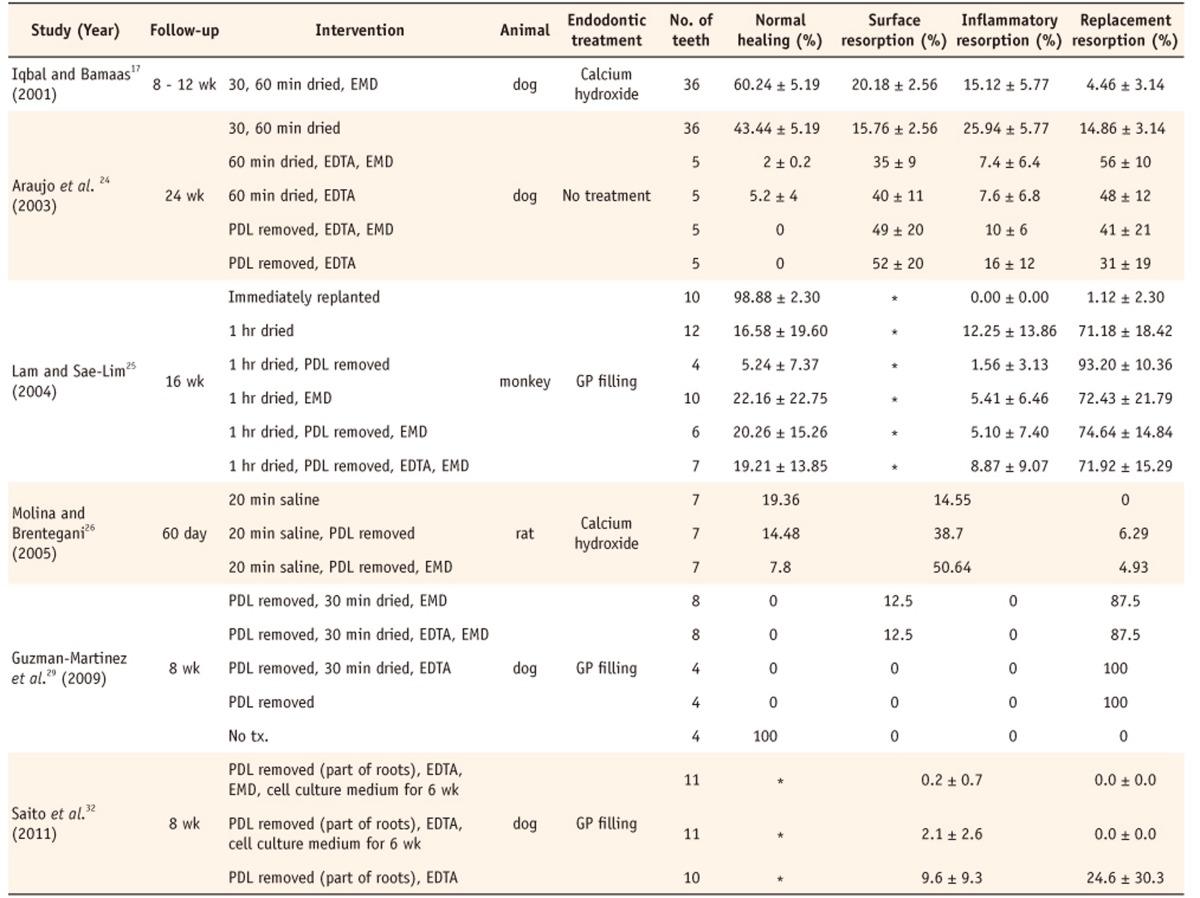
The characteristics of selected studies were summarized in Table 1.
Follow-up period: Follow-up periods approximately ranged from 8 to 24 weeks. One study used 7-, 20-, and 60-day follow-up periods.26
Extraoral time: Teeth were replanted after 20 - 60 minutes extraoral time, except for the study using a cell culture medium for 6 weeks before transplantation.32
Endodontic treatment: Teeth were endodontically treated and filled with calcium hydroxide or gutta percha root canal filling material prior to replantation in all studies except one study.17,19,24-26,32
Statistical analysis
The presence or absence of PDL prior to EMD application was considered to be the most significant factor in periodontal healing of replanted teeth. The studies were selected and arranged according to the presence or absence of PDL before EMD treatment for qualitative and quantitative analysis.
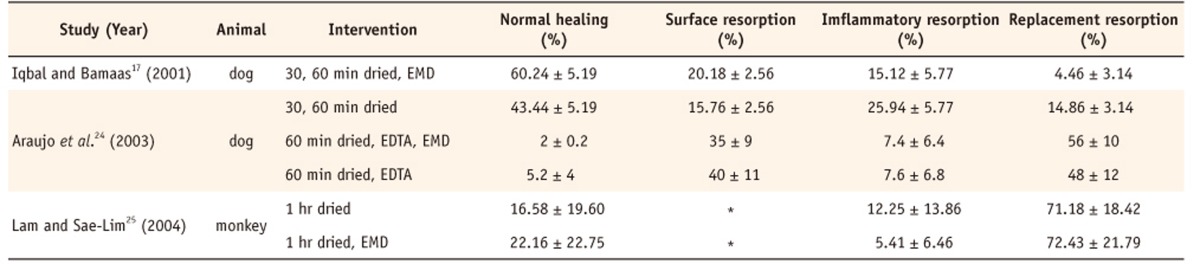
1. Presence of PDL
Three studies were selected for analysis as described in Table 2.17,24,25 Two studies17,24 were chosen for a meta-analysis because the other study25 did not have data for surface resorption and used different animal model (monkey). The meta-analysis was undertaken to produce a statistically more precise estimate on the effect of EMD on normal healing and root resorption in replanted teeth compared to the control. On the assumption that EDTA did not have a significant effect on healing and root resorption, the data were analyzed using the following outcome measures: normal periodontal healing, surface resorption, inflammatory resorption and replacement resorption.
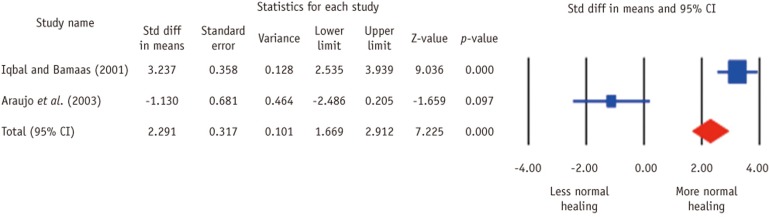
Normal healing. The pooled estimates showed a significantly higher normal healing in EMD-treated groups compared with non-EMD-treated groups (Z = 7.225, p < 0.001) (Figure 2). The heterogeneity among studies existed (Q = 32.205, df(Q) = 1, p < 0.001, I2 = 96.895).
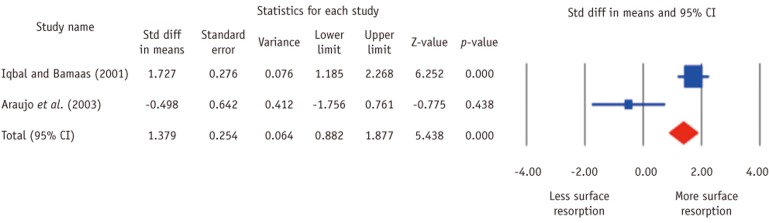
Surface resorption. The pooled estimates showed a significantly higher surface resorption in EMD-treated groups compared with non-EMD-treated groups (Z = 5.438, p < 0.001) (Figure 3). The heterogeneity among studies existed (Q = 10.123, df(Q) = 1, p = 0.001, I2 = 90.122).
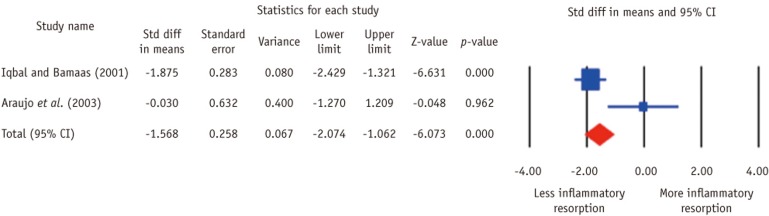
Inflammatory resorption. The pooled estimates showed a significant less inflammatory resorption in EMD-treated groups compared with non-EMD-treated groups (Z = -6.073, p < 0.001) (Figure 4). The heterogeneity among studies existed (Q = 7.091, df(Q) = 1, p = 0.008, I2 = 85.897).
Replacement resorption. The pooled estimates showed a significant less replacement resorption in EMD-treated groups compared with non-EMD-treated groups (Z = -7.437, p < 0.001) (Figure 5). The heterogeneity among studies existed (Q = 29.200, df(Q) = 1, p < 0.001, I2 = 96.575).
2. Absence of PDL
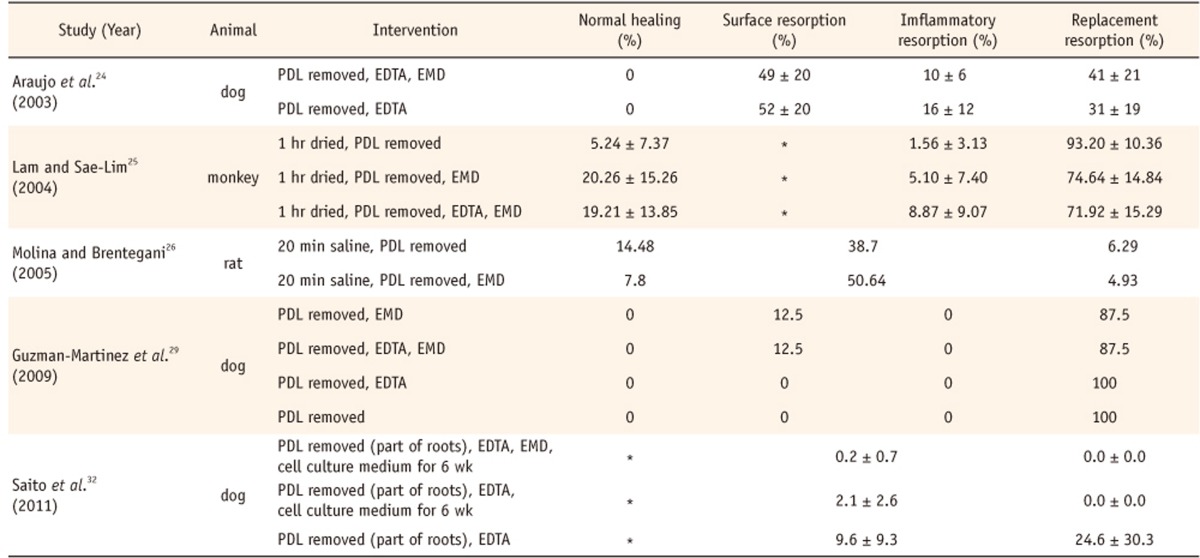
Five studies were selected for analysis as described in Table 3.24-26,29,32 Quantitative comparison of the studies could not be performed because there were missing data in our outcome categories, and no standard errors presented.25,26,29,32 Therefore, qualitative analysis was performed to assess the effect of EMD on periodontal healing and resorption in replanted teeth. There were no apparent differences in normal healing and root resorption between EMD-treated groups and non-EMD-treated groups irrespective of animal models in the included studies except for one study.32 In the study by Saito et al., EMD treatment showed significantly less surface and inflammatory root resorption (0.2 ± 0.7) compared with cell culture only group (2.1 ± 2.6) and control group (9.6 ± 9.3).32 Besides, replacement resorption was shown to be prevented significantly by EMD compared with control group.32 In this study it should be noted that only coronal part of PDL was removed before EMD application, and it was incubated in cell culture medium for 6 weeks to promote regeneration of PDL cells before tooth transplantation.32
Discussion
This systematic review aimed to investigate the effect of EMD treatment on periodontal healing in replanted teeth and to provide statistical evidence whether EMD treatment promotes healing and deters root resorption of replanted teeth compared to no EMD treatment. In this systematic review, a meta-analysis was performed to synthesize the evidence with a greater statistical power based on the effect size calculated from the individual studies. Two studies with similar study designs were selected for this statistical analysis, because the significant heterogeneity was found among the rest of studies, and thus, the inclusion of the heterogeneous studies would likely result in a less precise estimate.17,24 Only qualitative analyses could be performed for the comparison of the studies with significantly different study designs.
In this review, we hypothesized that the presence of PDL before EMD treatment could play a critical role in periodontal healing of replanted teeth. As was shown in the results of the meta-analysis, EMD treatment significantly reduced inflammatory and replacement root resorption and promoted normal periodontal healing as well as surface resorption when PDL existed prior to the treatment. On the other hand, it is difficult to have a definite conclusion about the effect of EMD on healing when PDL does not exist before EMD treatment because of the great heterogeneity of included studies, although it seemed that no apparent differences were found in normal healing and root resorption between EMD-treated groups and non-EMD-treated groups in general.
The heterogeneity of study designs among studies made it difficult to carry out the statistical analysis, although the studies with similar study designs could be identified and analyzed with a meta-analysis. There was a previous systematic review on the healing of replanted teeth with EMD treatment.30 However, no conclusion could be drawn due to the small number of studies and heterogeneous characteristics of included studies.30 In the present review, three additional studies met our inclusion criteria and included for final evaluation.24,29,32 Most of all, different animal models such as monkeys, dogs and rats were used in the included studies of the present systematic review. Histological data in one study could not be directly compared with that of other studies if different animal models were used because it is expected that healing time and pattern would vary among animal species.33,34 For example, dogs were known to have a faster bone turnover rate compared with non-human primates and rats.33,34 In this systematic review, a meta-analysis was carried out with data from two dog studies. Interestingly, these two studies showed very different periodontal healing outcomes in replanted teeth after EMD application. Iqbal and Bamaas showed that EMD significantly decreased replacement root resorption, while it promoted normal periodontal healing.17 No significant difference was found in the incidence of inflammatory and surface root resorption between EMD-treated groups and non-EMD-treated groups. On the other hand, Araujo et al. demonstrated that EMD could not increase favorable periodontal healing in replanted teeth.24 No significant difference was noted in normal periodontal healing and root resorption including surface, inflammatory and replacement root resorption.
According to the most recent guideline of International Association of Dental Traumatology, endodontic treatment needs to be performed 7 - 10 days after replantation of permanent teeth with closed apex.35 Calcium hydroxide followed by root canal filling is suggested to prevent inflammatory root resorption in replanted teeth.36 Most included studies in this present review appear to follow this guideline. Indeed, calcium hydroxide was placed as an intracanal medicament in two studies,17,26 and root canals were filled with gutta percha root filling materials in three studies.25,29,32 However, one study did not use any intracanal medicament or root canal filling material.24
Clinically, EMD has been recommended to stimulate periodontal cells to regain normal periodontal apparatus. It has been shown that no viable PDL cells existed in avulsed teeth when the extraoral time exceeded 60 minutes.37-39 Therefore, it is reasonable to assume that PDL removal in included studies can be interpreted as a clinical situation where a tooth was dried extraorally longer than 60 minutes. Based on the result of our meta-analysis, EMD appears to enhance normal periodontal healing and prevent inflammatory and replacement root resorption when the extraoral time is up to 60 minutes or less. In replanted teeth with extended extraoral time (> 60 minutes), EMD treatment might not be effective in promoting normal periodontal healing and preventing root resorption based on qualitative analysis, but no definite conclusion could be drawn due to the heterogeneity of the studies.
EDTA was known to demineralize the acellular cementum, expose collagen fibers on the root surface, and contribute to cell attachment and proliferation.40 In some studies, root surfaces were conditioned with 24% EDTA gel in the hope of promoting periodontal healing.24,25,29,32 However, the effect of EDTA on periodontal healing was not exhibited in our included studies. Araujo et al. showed that EDTA and EMD treatment group had similar amount of replacement root resorption to EDTA only group.24 Guzman-Martinez et al. also had no significant effect of EDTA on the replacement root resorption in replanted teeth.29 Similar findings were noted in a monkey study by Lam and Sae-Lim.25 Therefore, in the present systematic review, EDTA was not considered a critical variable when a meta-analysis was performed.25
The exact mechanism of EMD still remains unknown, while EMD has been clinically used to restore functional PDL, cementum, and alveolar bone. It has been proposed that amelogenin, a major component of EMD interacts with cells and induces the release of signaling molecules that secondarily initiates the regenerative process.41 EMD appears to stimulate the migration and proliferation of periodontal cells such as osteoblasts, endothelial cells and epithelial cells in vitro.42 Healing of the periodontal tissues in replanted teeth depends on the competitive cellular activities including the migration, attachment, proliferation and differentiation of various periodontal cells such as PDL cells, cementoblasts and osteoblasts. It is presumed that EMD could contribute to the favorable periodontal tissue regeneration in replanted teeth if the cell activities were harmoniously enhanced and controlled.41,43,44 More favorable outcome can be anticipated if there are viable PDL cells around the root surfaces of replanted teeth.
Despite the fact that a meta-analysis can be carried out with two studies, the results in this review should be interpreted with caution because any new studies may significantly influence the effect size.45 Further well-designed controlled studies are warranted to assess the effect of EMD on the periodontal healing in replanted teeth with a greater statistical power.
Conclusions
In our systematic review, it can be concluded that the treatment of EMD before replantation may be effective in enhancing normal healing and reducing inflammatory and replacement root resorption in the presence of PDL. In the absence of PDL, however, no clear relationship between EMD treatment and healing of replanted teeth could be determined because of the heterogeneity of the included studies.


 XML Download
XML Download