

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Polymerization shrinkage of adhesive restorative materials and the difference in the physical properties of the tooth structure and restorative materials are considered the most important factors in the microleakage formation of dentin-composite resin adhesive interfaces.1 In the case of a molar restoration with composite resin, resin modfied glass ionomer cements (RMGIC) are recommended as a base because the base materials with low elastic moduli can absorb polymerization shrinkage stress2,3 and the base materials can be used to reduce the mass of the restorations to reduce polymerization shrinkage.4 On the other hand, it is unclear if the use of RMGIC can prevent gap formation in dentin-restoration interfaces. This so-called sandwich technique has not been confirmed and some researchers have reported that this technique did not offer any added advantage5,6. Opdam et al. reported that a totaletch restoration with a highly filled hybrid composite resin showed a higher clinical survival rate than a closed-sandwich restoration.7 The main reason for failure in the glass ionomer (GIC) based composite restorations was a fracture of the composites, whereas Kwon et al. reported that the use of RMGIC as a base material can reduce a marginal defect in an overlying composite restoration when the elastic modulus of RMGIC was high.8
Hayashi and Wilson reported that marginal deterioration and cavo-marginal discoloration were significantly correlated with the clinical failure rate at the 5-year review.9 Souza-Junior et al. evaluated marginal and internal adaptation of restorations, in which internal adaptation were accessed by cutting the samples after marginal adaptations had been measured first.10 In their studies, internal gap formation was most prominent at the pulpal and axiopulpal line angle of restorations. The presence of gaps at these areas could cause fluid flow in dentin tubules, resulting in typical postoperative sensitivity.11 In addition, transudation of dentinal fluid through dentin adhesive could result in the water-filled regions, which could contribute to degeneration of adhesives.12 As for the internal adaptation of restorations, Ratih et al. reported in their fluid measurement and scanning electron microscopic study that the teeth restored with a high shrinkage composite demonstrated the greatest final volume of outward flow, whereas the group lined with RMGIC showed the lowest final volume and the gap between the dentin and restoration was most intimate.13 In contrast, in other studies, the internal adaptation of dentin-restoration interfaces was evaluated by fluid flow measurements,14,15 microgap analysis,14,16 and internal leakage measurements,14 and gap formation was observed frequently when RMGIC was used as a base.
Swept-source optical coherence tomography (SS-OCT) was applied to detect defects of restoration in cross cut image in real time.17 It successfully evaluate marginal gaps, internal porosities and defects. However, it did not differentiate whether radiolucency between composite restoration and tooth was due to defective bonding or it was just image of normal bonding agent.
Some studies employed micro-CT to analyze the adaptation between the tooth and restorative materials. Some researchers reported that micro-CT was a powerful tool for quantifying polymerization shrinkage and corresponding microleakage.18,19 Kakaboura et al. evaluated the adaptation of composite resins to dentin versus the shrinkage strain of the composites.20 They reported that there was a positive correlation between the setting shrinkage and interfacial gap volume at the bottom sites of the composite restoration due to differential shrinkage. On the other hand, these studies may not be relevant to a clinical situation because the composites were placed in a cavity without adhesives. Eden et al. prepared standard class II cavities in 14 primary teeth and restored them with composite resin and adhesive.21 The teeth were then immersed in 50% silver nitrate solution for 4 hours and the penetration depth was measured with micro-CT. That study successfully analyze non-destructively the marginal adaptation of composite resin adhesive interfaces to enamel and dentin, but it did not evaluate the internal adaptation inside the restorations. In the present study, the initial internal adaptation of dentin-composite resin adhesive interfaces with or without RMGICs, and the degree of destruction of internal adaptation by mechanical loading were analyzed non-destructively using micro-CT and a silver nitrate solution.
Materials and Methods
Specimen Preparation
Thirty intact human premolars or molars extracted within a month for orthodontic treatment were used. A high speed diamond bur was used to amputate the roots from the cervical regions and 3 mm (bucco-lingual) × 3 mm (mesiodistal) × 4 mm (depth) class I cavities were prepared. Using digital radiographs and its software, the distance between the cavity floors and pulp chambers was controlled within 1.0 mm. Thirty specimens were divided randomly into 3 groups.
1) Control group
The interior parts of the cavities were etched with 10% phosphoric acid (ALL-ETCH, Bisco Inc., Shaumburg, IL, USA) for 15 seconds. During the etching process, enamel was agitated with a minibrush, whereas dentin was not. Composite resin (Tetric N-Ceram, Ivoclar Vivadent, Schaan, Lietchtestein) was filled into the cavity without an adhesive. The cavity was filled 2 mm at each time using an incremental technique. In each increment, the composite was light cured for 20 seconds using an LED type light curing unit (Bluephase, Ivoclar Vivadent).
2) Group 1 (base group)
After a conditioner (DENTIN CONDITIONER, GC, Tokyo, Japan) was applied to the interior parts of the cavities for 20 seconds, it was irrigated and dried gently. Care was taken not to dry the exposed dentin surface too much because. Then, base layers, the thicknesses of which were 2 mm, were formed using light cured GIC (Fuji II LC, GC, Tokyo, Japan). The cavities were then processed with 10% phosphoric acid for 15 seconds, and washed and blot dried. The dentin adhesive (All-bond II, Bisco Inc.) was applied according to the manufacturer's recommendations, and cured for 20 seconds using a LED type light curing unit. The same composite resin as the control group was applied 2 mm each time using an incremental technique. The resin was cured with the LED type light curing unit for 20 seconds.
Pre-loading a silver nitrate solution application
The pulp chambers were soaked with 17% Ethylenediamine tetraacetic acid (EDTA) for 5 minutes. They were then washed with saline. The teeth were immersed in 25% silver nitrate solution and were under a pressure of 3 kgf for 3 days.
Pre-loading micro-CT taking
High resolution micro-CT (Model 1076, SkyScan, Aartselaar, Belgium) was used to take photographs under the conditions of 100 kV acceleration voltage, 100 µA beam current, 0.5 mm Al filter, 18 µm resolution and 360° rotation at 0.5° step. Two dimensional images of 550 - 560 sagittal and coronal of each specimen were taken. During this procedure, the tooth specimen was mounted in a special template that was made purely for that specimen. This template minimizes the change in the position of the specimen during repeated use in the process. The 2D images were analyzed using the CTAn (SkyScan, Aartselaar, Belgium) program.
Application of mechanical loading by a chewing simulator
A custom made chewing simulator was used to apply a mechanical load of 5 kgf (- 49 N) for 640,000 times under a continuous water flow. The conical-shaped opposing plunger, which was made of nickel-chromium, was initially positioned at the center of restorations, and vertical force was applied about 2 mm above the restoration through long axis of tooth crown.
Post-loading silver nitrate solution application
Using the same methods employed in pre-loading silver nitrate solution application, the silver nitrate solution was applied to the specimen after being loaded.
Post-loading micro-CT taking and analysis by micro-CT
The specimen was analyzed by micro-CT using the same method as in pre-loading. The 2D images were analyzed using the CTAn program .
Internal adaptation measurements
Among the 2D images of each specimen, 100 images clearly confirming the relationship between the pulpal floors and silver nitrate solution based on the central regions of the disto-mesial distances of cavities were selected. For the same specimen, a selection of 2D images before and after mechanical loading was made by choosing 100 cuts of 2D images arranged at equal intervals beginning from the initially photographed 2D image of a tooth. The silver nitrate penetration into the microgap between the tooth and restorative materials was considered to be valid when the densities were over 141 index, which was based on the observation that the parts clearly penetrated by the silver nitrate solution had densities > 141 index when the sagittal and coronal images (Figures 1a and 1b) of the same phase were compared. For each specimen, the length of the margin of the pulpal floor showing a microgap or intact margin was calculated in each image, and all the data was collected and summed. The ratio of the silver nitrate penetration length into the micro gap between the tooth and restoration with regard to the entire length of the pulpal floor was calculated for each specimen (% SNPL). In this way, 100 datum points were collected for each specimen and the mean % SNPL was calculated. For each group, the data of 10 specimens were collected in the same manner.
Statistical Analysis
One-way ANOVA was used to compare the % SNPL between the groups before and after loading, respectively. A paired t-test was used to compare the % SNPL before and after mechanical loading. Duncan analysis was used for post hoc analysis. All statistical inferences are made within a 95% confidence interval.
Results
General aspects of silver nitrate penetration
Generally, the silver nitrate solution successfully penetrated into the dentinal tubules from the pulp spaces, and infiltrated into the gap between restoration and pulpal floor.
In control group, silver nitrate solution was distributed uniformly throughout the entire pulpal floors of the teeth in a control group (Figure 2a). The amount of silver nitrate penetration increased after mechanical loading. In addition, a silver nitrate solution primarily penetrated the axio-pulpal line angle regions (Figure 2b).
In group 1, a few air bubbles were observed inside the base materials and gaps were visible around the axiopulpal line angle regions. In a comparison with other groups, silver nitrate penetration was concentrated in the axiopulpal line angle regions. Even before mechanical loading, a large amount of a silver nitrate solution penetrated the specimens (Figure 3a), but a change in the penetration quantities after mechanical loading appeared to be smaller than in the control group (Figure 3b).
In group 2, before loading, a thin radiolucent line, which was assumed to be dentin adhesive, was present between the composite resin restorations and cavity floors. This line was thicker in the cavity corner than in the middle part of the cavity. After loading, the line appeared to be affected more by silver nitrate. The level of silver nitrate penetration (Figure 4a) and the change between before and after mechanical loading appeared to be smaller than in the control group (Figure 4b).
% SNPL evaluation
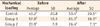
Table 1 lists the mean % SNPL and standard deviations. Group 2 showed a lower % SNPL than the control group and group 1 (p < 0.05). There was no significant difference between the control group and group 1. In all groups, there was a significant difference between before and after mechanical loading (p < 0.05).
Discussion
In a pilot study which was done before this experiment, the appropriate silver nitrate concentration enabling adequate radiopacity and permeation through the dentinal tubules was studied. In addition, tooth preparation methods, the use of pressure and acid conditioning in the pulp space to enhance the penetration of silver nitrate solution from the pulp space to the gap spaces between the restoration and cavity floor were tested under many conditions. In this pretest, when the distance between the cavity floor and pulp chamber was within 1 mm, the pulp chamber was soaked with 17% EDTA for 5 minutes, and a 25% silver nitrate solution was allowed to penetrate from the pulp space to the pulpal floor of the cavity under a pressure of 3 kgf for 3 days, the silver nitrate solution could fill the gap between the teeth and restoration successfully and provided adequate radiopacity. These experimental conditions were applied in the present study. Even though it is very difficult for silver nitrate solution to penetrate deeply into gap spaces, it successfully penetrated into the dentinal tubules from the pulp spaces, and infiltrated into the gap between restoration and pulpal floor in all samples.
Before mechanical loading, % SNPL might show the internal adaptation of the initial conditions. The control group and Group 1 showed a higher % SNPL than group 2 and there was no significant difference between the control group and group 1. Many studies reported that adaptations between the tooth and glass ionomer were poor.14-16,22 Composite resin restorations with bases had inferior internal adaptation because of the porosity of light-cured GIC14 and polymerization shrinkage of the composite resin and light-cured GIC.15,23,24 The 2D image of group 1 showed many air bubbles (Figures 3a and 3b). These porocities might be incorporated during the mixing procedure of the light-cured GIC powder and solution, which could promote fluid storage and accelerate micro-gap formation.25 In the present study, as the GICs were hand mixed, more favorable results would be expected when encapsulated materials would be used. It needs further research.
During polymerization, a composite resin develops contraction force and the shear bond strength that can resist this contraction force and stop micro-gap formation was reported to be 17 - 21 MPa.26 The bond strength between the light-cured GIC and dentin is relatively low, 5 - 10 MPa,27 whereas the shear bond strength between dentin and dentin adhesives was reported to be 21 - 29 MPa.28-31 When a light cured glass ionomer is used as the base material in composite restoration, it is believed that the HEMA components of light-cured GIC form chemical bonds with the composites.32 Therefore, the micro gap in group 1 might be developed during the polymerization stage because the composites might pull up the light cured glass ionomer during the course of polymerization. When traditional GIC was used as a base and composite resin was used for the restoration, traditional GIC formed smaller micro-gaps with the dentin and larger micro-gaps with the composite resin than light-cured GIC.14 This outcome can be explained by the fact that during polymerization shrinkage of composite resin, gaps are formed between the composite resin and traditional GIC because of its lower bonding strength with the composite resin compared to that of light-cured GIC and thus stress is not transmitted to traditional GIC.24 In the present study, however, a relatively thick, 2-mm base material, Fuji II LC, was placed. The elastic modulus of Fuji II LC (6.2 - 10.8 GPa)33 is higher than that of the other light cured glass ionomer base materials, such as Vitrabond (1.1 GPa)34 and GC Lining Cement (2.9 GPa).35 The base thickness and relatively high elastic modulus of the base material might reduce the internal gaps better than the other GIC.
Polymerization shrinkage of light-cured GIC itself might be one of causes of the poor adaptation to dentin interfaces.24 Polymerization shrinkage of light-cured GIC was reported to be lower than that of the composites partly because GIC absorbs moisture and expands, thereby compensating for polymerization shrinkage.36 When light-cured GIC is used as a base, the composites on the top of the base completely exclude external moisture and only dentinal tubule fluid originating from the pulp chamber provides moisture. In the present study, the pulp chamber was removed from the extracted teeth, and the source of moisture was eliminated completely. Therefore, the light-cured GICs used as a base were self-dried and unable to compensate for polymerization shrinkage.37 Comparative analysis of internal adaptation showed that the vital teeth restored with composite resin, and light-cured GIC as bases showed superior internal adaptation but the extracted teeth with the same restorations had multiple microgaps.38 As GIC is a water-based material, it may be more likely to take up silver nitrate in the water component and porosities would be quickly filled with the silver nitrate solution, which does not represent the reality of degree of leakage/gap formation. It will also need further research.
When glass ionomers were used as base materials, the hypersensitivity after posterior composite restorations was reported to be reduced39 or at least comparable to restorations filled with the composites only.40,41 Unemori et al. reported that the postoperative sensitivity in the resin composite restorations was not related to the absence of protective layers but increased with the depth of the cavities restored with the resin composite and type of dentine-bonding.41 The internal adaptation of GIC was poor. Therefore, the internal adaptation of the base material may not affect the post operative sensitivity. In a 2D image of group 1, microgaps were formed in the axio-pulpal line angle areas of the light-cured GIC (Figures 3a and 3b). This is consistent with a previous study, which reported that polymerization shrinkage stress was concentrated mainly in the axio-pulpal line angle regions of the restoration-detin interfaces. As a result, micro-gaps were formed in those regions by a photoelastic model after restoring the teeth with composite resin, and light-cured GIC as bases.24
In group 2, the % SNPL was lower than the other groups. This might be related to the strong bonding strength of the dentin adhesives resisting the contraction force of composite resin polymerization.15 All the groups showed significant differences in %SNPL between before and after mechanical loading. In the present study, a chewing simulator was used to compare the extent of destruction of internal adaptation. Although there is some dispute as to whether the chewing simulator can mimic the long term clinical conditions,42 it would be possible to use it to evaluate the effect on the restoration after mechanical loading. In this study, thermocyling was not applied based on the study by Heintze et al., who reported that it had a slight effect on marginal adaptation, whereas mechanical loading had a significant effect.43
Before the length measurement, the Data Viewer (SkyScan) program was used to measure the densities of dentin, restorations and silver nitrate. The measured densities were 40 - 65 for dentin, 60 - 75 for light-cured GIC, 90 - 130 for the composite resin, and 125 - 180 for silver nitrate. In the present study, some light cured glass ionomers that showed a similar density to dentin were excluded, and Fuji II LC was selected because a restoration material with a similar radio-density to dentin might show background noise.44 In the present study, silver nitrate penetration into the microgap between the tooth and restorative materials was considered to be valid when the densities were > 141 index. This was based on the observation of pilot studies that the parts clearly penetrated by a silver nitrate solution had densities > 141 index when sagittal and coronal images of the same phase were compared. The index may vary in other studies because the radiodensities can differ according to the silver nitrate solution concentration and loading periods. Even though evaluating the marginal adaptation between enamel and composite was not the purpose of the present study, we could not observe any significant silver nitrate penetration in this area. In a very few cases, there were only a slight infiltration less than 100 µm. Therefore, the possibility that silver nitrate penetrated into internal gap from marginal gap seems to be very low.
In the present study, the same samples, which were used for pre-loading test, were used for post-loading test. To analyze the % SNPL after loading, the silver nitrate solution was applied to the specimen once again after being loaded using the same methods employed in preloading silver nitrate solution application. In the pilot study of this experiment, when the silver nitrate solution was not additionally applied for the after-loading analysis, the penetration of it was the same as that of pre-loading data. It means there was no further movement of silver nitrate solution after the pre load analysis. The silver nitrate may stick to the tooth substance once it contact with it. That was the reason why another silver nitrate solution was applied for post-loading test.
Overall, the method using micro-CT and a silver nitrate solution was effective in the non destructive analysis of internal adaptation between restorations and dentin. For further study, comparing the data with that of conventional sectioning or SS-OCT is necessary to corroborate the outcomes as this experiment.
Conclusions
The internal adaptation between dentin and restorative materials before and after loading was better when composites were bonded to tooth using adhesive agent than composites based with RMGIC. The proposed method, in which a silver nitrate solution was penetrated from the pulp space through the dentinal tubules and the amount of silver nitrate penetration in micro-gap areas was assessed by micro-CT, may provide a new measure for evaluating the internal adaptation non-destructively, but comparing the data with that of conventional sectioning seems to be necessary.




 XML Download
XML Download