

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Trauma to the facial area generally involves the teeth and their supporting structures, and the fractures of permanent teeth comprise the most frequent type of dental trauma.1 The teeth most commonly involved are the maxillary incisors and the these injuries can be characterized by tooth avulsion and coronal fracture with or without pulp exposure. Crown fracture with pulp exposure represents 18 - 20% of traumatic injuries involving the teeth, the majority being in young permanent teeth.2
Reattachment technique has been published since 1964, when Chosak and Eidelman reported a case that involved reattaching the natural fragment of incisors.1 As adhesive dentistry developed, the incidence for choosing crown reattachment as the first choice of treatment for restoring fractured teeth is increasing. This crown reattachment technique has several advantages. It is the most conservative treatment, thus it maintains the original contour and incisal translucency. In addition, less chair time is required, which reduces the cost of the treatment.3
However, in crown fractures accompanied by a pulp exposure, we should consider the following treatment option of the pulp: pulp capping, pulpotomy, and pulpectomy. We should try to plan the ideal procedure not only to get a good bonding of the fragment but also to minimize the pulpal irritation during the whole procedure. This case reports a crown fracture case with pin-point pulp exposure that was treated using crown reattachment with direct pulp capping.
Case report
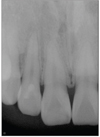
A 26-year-old woman visited the department of conservative dentistry because of crown fracture of the right central and lateral incisors after falling down in the bathroom twenty minutes before arriving at the dental office. The patient found tooth fragments and brought them stored in milk. Clinical and radiographic examination revealed that those two teeth were fractured supragingivally involving a pin-point exposure of the pulp (Figure 1). Because the pulp exposure size was minimal and exposure time was of short duration, crown fragment reattachment with direct pulp capping was planned.
In order to avoid the pulpal contamination, the area was carefully irrigated with chlorhexidine and normal saline under rubber dam isolation. For hemostasis of the exposed pulp, cotton pellet with 2.5% sodium hypochlorite was pressed gently against the lesion.4 After complete hemostasis was confirmed, the exposed pulp was covered with sterile cotton pellet in order to avoiding direct contact with acid. Enamel was etched with 35% phosphoric acid gel for 30 seconds.5 After rinsing and drying, the exposed pulp was capped with calcium hydroxide (Dycal, Dentsply Caulk, Milford, DE, USA) (Figure 2).
After setting of Dycal, Clearfil SE bond(Kuraray Medical Inc, Okayama, Japan) was applied following the manufacturer's instruction. To avoid dehydration during clinical procedure the tooth fragment were immersed in saline solution. Tooth fragment was acid etched using 37% phosphoric acid (Bisco, Schaumberg, IL, USA) for 30 seconds. The acid was eliminated by rinsing with copious water and drying with gentle air. Clearfil SE bond was applied in the same manner above. After bonding, Aelite flow A2 shade (Bisco) was used to reattach the fragment to the remaining teeth. Flowable resin was light cured for 40 seconds each from the labial and palatal directions (Figure 3). The residual excess resin at the tooth surface and irregular margin surface was left untouched without finishing and polishing.
Four days later, fracture line reinforcement and polishing was done. After shade selection (Figure 4), preparation was placed on the buccal and palatal surface extending 2.5 mm coronally and apically from the fracture line with a depth of 0.3 mm (Figure 5). The area around fracture line was acid etched using 37% phosphoric acid (Figure 6). Then, adhesive was applied and light cured, followed by placement of resin composite to create slightly overcontoured surface. Excess composite resin was removed and polished (Figure 7). Periapical view showed no periodontal or periapical pathosis (Figure 8).
After 14 months, patient showed no clinical symptoms and the vitalities were well maintained. In addition, radiographic examination showed normal condition (Figure 9). The crowns were functionally and esthetically acceptable.
Discussion
Some previous case reports showed that tooth fragment reattachment is an alternative for restoring aesthetics and function of the injured teeth with or without pulp exposure.1,6-8 In case of crown fractures with pin-point pulp exposure, we should be concerned about the pulpal status and pulp capping materials during crown reattachment procedures. Therefore unlike conventional crown reattachment technique of the fractured tooth without pulp exposure, this procedure has several different clinical steps. Especially, we should consider the etching, primer application, and polishing steps. The following considerations are presented for the best functional and esthetic outcomes.
First of all, we should consider the acid etching step. As in the current case, if the pulp is minimally exposed, acidic etchant should not be in direct contact with pulp. Pameijer and Stanley reported that if acidic etchant came in contact with the exposed pulp, hemostatic effectiveness and resin sealing was greatly reduced.9 Thus, in this case, acidic etchant was applied to the enamel surface only. Also the exposed pulp was covered with sterile cotton pellet in order to avoid direct contact with acid.
Then, etching procedure was done after Dycal setting in order to prevent pulpal damage from acid etching, we wonder if it is better. Burke and Watts reported that during an etching and washing cycle, Dycal lost 14.4% of its mass.10 The loss of material from Dycal as a result of acid contact is generally regarded as disadvantageous. Therefore, etching procedure should be done before Dycal application.
Second, primer selection is important. El-Araby and Al-Jabab reported that some primers contain acetone or alcohol that may affect the properties of Dycal which is placed for direct pulp capping.11 In this article, Dycal treated with Scotchbond multipurpose (3M Dental Products, St. Paul, MN, USA), Singlebond (3M Dental Products), and Gluma CPs (Heraeus Kulzer, Dormagen, Germany) had the lowest erosion values and the highest compressive strength value. These materials are water-based primers. Clearfil SE bond used in this case is also a water-based primer. Therefore, direct pulp capping using Dycal with subsequent sealing with water-based primer may show favorable results in pulp tissue.
Finally, timing of polishing should be considered. Conventionally, polishing and reinforcement of fracture line is done immediately after the fragment is rebonded in a single visit. However, Macedo and Ritter reported that delaying the overcontouring of fracture line is better to reduce the repeated pulpal damage in case of tooth treated by direct pulp capping because force and heat generated from preparation and polishing step may affect the pulpal status.8 Therefore, in this case, crown reattachment was done immediately but fracture line preparation, overcontouring and polishing steps were delayed 4 days after reattachment.
Conclusions
During the crown reattachment procedure of the fractured tooth with pin-point pulp exposure, we would recommend the followings:
First, acid etchant should not come in direct contact with pulp. Second, before Dycal application, etching procedure should be done. Third, direct pulp capping with Dycal and subsequent sealing with water-based primer may show favorable results in pulp tissue. Finally, delaying the preparation and polishing step is better to reduce repeated pulpal damage.








 XML Download
XML Download