

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A well-known cause for endodontic failure is the presence of untreated canals.1 Therefore, a thorough knowledge of root canal morphology and its variations is very important for a successful endodontic treatment. Many studies have described different root canal morphologies of maxillary molars.2-4 Some of these variations in morphology are related to the presence of a C-shaped root canal in the maxillary first molars rather than in the mandibular second molars where such a variation is commonly observed.2,5,6
Although conventional radiographic examination provides essential information for the successful management of endodontic problems, this technique has many limitations, which mainly results from superimposition of structures.7 Cone-beam computed tomography (CBCT) overcomes these limitations by providing a three-dimensional image of the object.8 Therefore, CBCT is an important tool for identifying the configuration of root canal systems that enables a successful endodontic treatment, especially in the case of teeth with complex root canal morphology.9-11
Although some studies have reported C-shaped root canals in maxillary molars, to our knowledge, few studies have described the C-shaped root canal configuration in a maxillary first molar involving 3 independent buccal canals, and none of these findings were confirmed by CBCT.12 Our case report describes the endodontic management of a maxillary first molar with a C-shaped root canal configuration of the 3 independent buccal canals confirmed by CBCT.
Case report
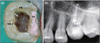
A 26-year-old woman was referred from a private dental clinic to Wonkwang University Dental Hospital for root canal treatment of maxillary left first molar. The patient's medical history was noncontributory. Medical history revealed spontaneous pain on the upper left side of her face for the past several days. Clinical examination showed a large distal temporary restoration and tenderness to percussion on the maxillary left first molar. Diagnostic radiograph showed the presence of subgingival caries in the distal area of the tooth (Figure 1a). On the basis of clinical and radiographic examination, the patient's condition was diagnosed as pulp necrosis with acute apical periodontitis and endodontic treatment was recommended.
After profound anesthesia and rubber dam isolation, temporary restoration was removed. The pulp chamber was rinsed using 2.5% sodium hypochlorite. The evaluation of pulpal floor using an endodontic explorer revealed only 2 obvious canal orifices: mesiobuccal and palatal. Working length of the mesiobuccal and palatal canals was determined using an apex locator (Root ZX, Morita, Tokyo, Japan). The radiograph for determining the working length indicated a possibility of furcal perforation on buccal root (Figure 1b). To rule out the occurrence of perforation and the presence of any additional roots/canals, CBCT imaging of the tooth was performed. Informed consent was obtained from the patient, and a CBCT of the tooth was performed (Alphard VEGA, Asahi Roentgen Ind. Co., Kyoto, Japan) using a tube voltage of 80 kV and tube current of 8 mA. We used the D mode of the CBCT, which has the smallest field of view (FOV) covering only 2 to 3 teeth. All protective measures were taken to protect the patient from scattered radiation. Transverse slices of the tooth were obtained at different levels to determine the mesiobuccal and distobuccal canal morphology (Figure 2). The buccal root showed 3 root canals in the C-shaped root that extended from the cervical third up to the junction of the middle and apical third.
Endodontic ultrasonic tips (CPR tips, Spartan, Fenton, MO, USA) used for eliminating pulp stones and obstructions under dental operating microscope (OPMI pico Dental Microscope, Carl Zeiss, Oberkochen, Germany) revealed mesiolingual and distobuccal canals (Figure 3a). Working length was estimated by using electronic apex locator (Root ZX) and was confirmed using a radiograph. All the 4 canals were prepared using ProTaper nickel-titanium rotary instruments (Dentsply-Maillefer, Ballaigues, Switzerland) and irrigated using 2.5% sodium hypochlorite (NaOCl) solution.
At the next appointment, the canal system was irrigated using 17% ethylenediaminetetraacetic acid (EDTA) solution for 1 min, and then soaked using NaOCl solution for 30 minutes prior to obturation for control the debris may exist within isthmus between the buccal canals. Then, the canals were dried and obturated by using warm vertical compaction technique. A final radiographic examination confirmed the accuracy of the endodontic treatment and the presence of 3 different apical foramina for each of the buccal canals (Figure 3b).
Discussion
The C-shaped configuration refers to a continuous slit between all the canals so that a horizontal section through the root yields a space in the shape of the letter C.13 This variation is a result of the lack of division of the roots, which leads to a communication between the root canals, which may extend up to the apical third of the canals.5,14 Cooke and Cox described the C-shaped configuration in mandibular molars for the first time.15 Although this variation is most commonly found in mandibular second molars, its presence was reported in maxillary first molars, with the first case being reported by Newton and McDonalds in 1984.5,16,17 De Moor in 2002 further investigated the incidence of C-shaped root canals in maxillary first molars and concluded that the incidence was 0.091% and that the most common type is the fusion of distobuccal and palatal root.18 In our case report, however, the C-shaped canal results from the fusion of the distobuccal and mesiobuccal root. Furthermore, the C-shaped canal contains 3 independent canals, including mesiobuccal, mesiolingual, and distobuccal canals.
In the present case, the C-shaped canal system of the maxillary first molar was identified by CBCT. Although conventional radiograph is commonly used, it does not provide sufficient information about complex canal system morphologies.7 Therefore, a three-dimensional examination is beneficial to thoroughly understand complex anatomical morphologies such as a C-shaped canal configuration.19 Three-dimensional examinations have been performed previously to diagnose the conditions related to the anatomy of maxillary molars. Singla and Aggarwal used a spiral CT to report a C-shaped canal involving 2 different canals in the palatal root of a maxillary second molar.20 Recently, Kottoor and colleagues used CBCT to identify the apical third of the palatal root bifurcated into 2 different palatal roots similar to that in the case of our patient.21 In the case of our patient, CBCT images provided valuable information about the canal/root configuration and confirmed the presence of 4 canals and the relationship of the unusual C-shaped canal with the 3 buccal canals, which were not clearly visualized in the diagnostic periapical radiograph. Furthermore, unusual root/canal systems carry an increased risk of iatrogenic events such as root perforation.22 The presence of concavities on palatal or lingual root surface of a C-shaped root increases the risk of perforation.23 Thus, the use of diagnostic procedures such as CBCT might help in avoiding tragic results during canal preparation.
Whenever a clinician decides to acquire CBCT images, the risk and benefit of radiation should be considered. Generally, the radiation doses from CBCT are much higher than those in conventional periapical radiography. However, we used the D-mode (FOV, 51 × 51 mm) of the CBCT scanner that is similar in size to a conventional periapical radiograph. Compared to other modes of the CBCT scanner, such as the I-mode (FOV, 102 × 102 mm), P-mode (FOV, 169 × 119 mm), and C-mode (FOV, 200 × 179 mm), the D-mode has the smallest FOV. Patel et al. reviewed that the effective dose of a small FOV is 2 - 3 times higher than the FOV of a periapical film.24 Even though the radiation dose is relatively low, however, clinicians should consider taking CBCT only in limited situations based on ALARA (as low as reasonably achievable) principle recommended in radiology textbook.25
Conclusions
Taken together, two important aspects are highlighted in our case report. First, we have described a unique C-shaped variation of the root canal system in a maxillary molar. The C-shaped canals involve 3 buccal canals (mesiobuccal, second mesiobuccal, and distobuccal) of the maxillary molar, which, to our knowledge, has not been reported in many studies. Second, our study emphasizes the utility of CBCT as a very convenient diagnostic tool in patients with complex root anatomy for an endodontic treatment.


 XML Download
XML Download