

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In end-stage renal disease (ESRD) patients, the most common cause of death is cardiovascular disease1), because of advanced atherosclerosis in this population. Atherosclerosis progresses through two key elements, thickening (atherosis) and stiffening (sclerosis) of the arterial wall2). Arterial thickening causes ischemia and/or infarction and stiffening of arterial walls is associated with arterial dilatation and hypertrophy3). Atherosis of arterial wall has been considered as a risk factor of cardiovascular disease traditionally. Compared with atherotic change, sclerotic change of the arterial wall has only recently been studied. Arterial stiffness, a powerful independent predictor of all cause and cardiovascular mortality, can be examined by measurement of pulse wave velocity (PWV)4). Therefore, through the identification of high risk groups of cardiovascular disease in ESRD patients is by PWV, mortality rates can be decreased through early intervention. PWV had been traditionally computed on the basis of pulse transit time and the distance traveled between the carotid artery and femoral artery, i.e., carotid-femoral PWV (cfPWV). However this technique is complex and inconvenient, particularly in screening large populations. BaPWV appears equal in the efficacy for determining mortality to cfPWV in ESRD patients5). Recently a device assessing brachial-ankle PWV (baPWV) was developed. This technique using the device is more feasible for screening a large population than previous methods because of technical simplicity and convenience6, 7). Few studies have examined the baPWV and its influent factors in Korean ESRD patients. We conducted this study to evaluate the clinical factors associated with baPWV in patients on maintenance hemodialysis.
Methods
1. Subjects
This study is a cross-sectional study. Sixty-five ESRD patients who were undergoing maintenance hemodialysis therapy in Hanyang University Guri Hospital were recruited between February 2005 and June 2005.
2. Data collection
Demographic and medical data, including smoking habits, medication history, and cause of ESRD, were obtained from medical records and interviews. We classified patients with a smoking history of more than 20 pack-years as the smoking group, taking renin angiotensin system (RAS) blockade for more than 6 months as the RAS blockade group, and statin for more than 1 month as the statin group.
3. Physiological data and blood pressue measurement
All participants measured their height and weight after hemodialysis. Dry weight was assessed in a normal albumin level and just prior to manifest hypotension, muscle cramps, and postural hypotension clinically8).
Body mass index (BMI) and body surface area (BSA) were calculated from measured height and body mass using the following equation : BMI body mass (kg)/height (m)2, BSA (m2) = 0.20247×height (m)0.725×weight (kg)0.425. Interdialytic weight gain was adjusted by BSA. Blood pressure (BP) was assessed after 15 minutes of resting in the arm contralateral to the arteriovenous fistula with a mercury sphygmomanometer and a cuff of appropriate size. The mean arterial pressure (MAP) was calculated as the following equation: MAP = DBP+[(SBP-DBP)/3], where DBP and SBP represent diastolic blood pressure and systolic blood pressure, respectively. A total of eight measurements were made at predialysis and postdialysis. Pulse pressure was defined as the difference between SBP and DBP. ΔSBP, ΔDBP, and ΔMAP were defined as the difference between predialysis and postdialysis measurements of SBP, DBP, and MAP.
3. Laboratory measurements
Plasma total cholesterol, high-density lipoprotein cholesterol, triglycerides, uric acid, blood sugar, and serum creatinine levels were measured enzymatically. All blood samples were obtained in a fasting state in the morning.
4. Echocardiography
Two-dimensional M-mode echocardiography was performed by an experienced echocardiographer using the HP sonos 2,500. Left ventricular internal diameter (LVID), septal wall thickness (SWT), and the posterior wall thickness (PWT) were made according to the recommendations of the American Society of Echocardiography. Left ventricular (LV) mass was calculated using Devereux's formula : LV mass (g) = 0.80×[1.04×{(PWT+LVID+SWT)3-LVID3}]+0.69).
The LV mass index was performed by adjusting LV mass for BSA.
5. Measurement of baPWV
BaPWV and Ankle-brachial blood pressure index (ABPI) were assessed by using a Colin Waveform analyzer (form PWV/ABI; Colin, Co., Ltd., Komaki, Japan) which simultaneously records bilateral arm and ankle blood pressure, pulse volumes of brachial and posterior tibial arteries, heart sounds, and electrocardiogram. All patients were examined on supine position after hemodialysis treatment and after resting for their BP stabilized for at least 5 minutes. Monitoring cuffs were placed around both the brachium without blood access and ankles.
Results
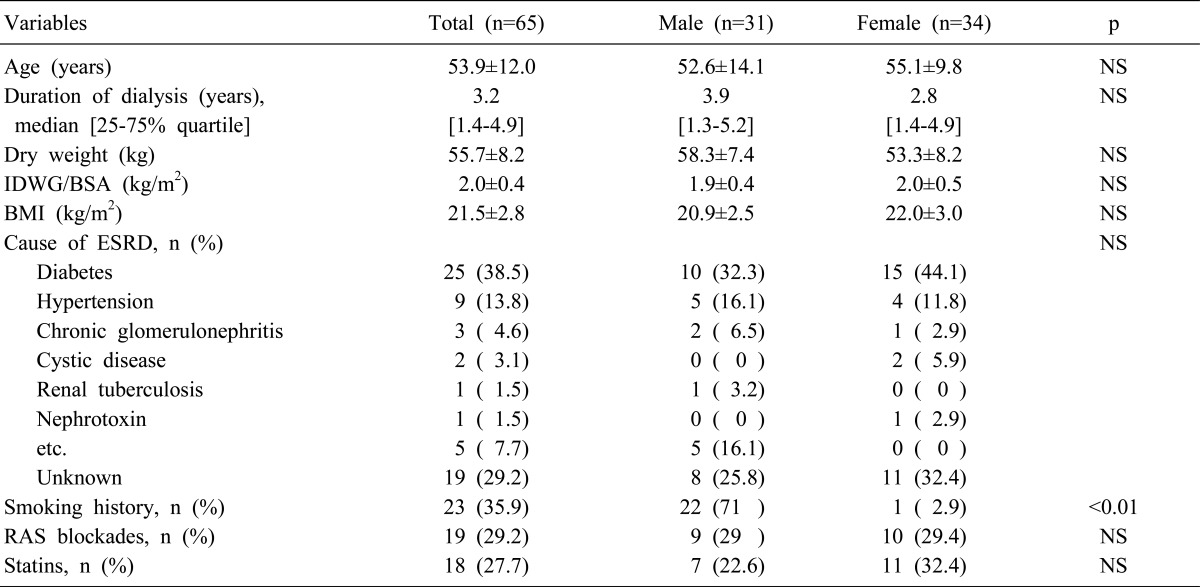
The clinical characteristics of study patients are shown in Table 1. Mean age was 53.9±12.0 years and dialysis duration was 3.2 (25-75% quartile, 1.4-4.9) years. The causes of ESRD included diabetes, hypertension, chronic glomerulonephritis, etc. In 29.2% of the patients, the cause was not identified. These characteristics were not different between both genders.
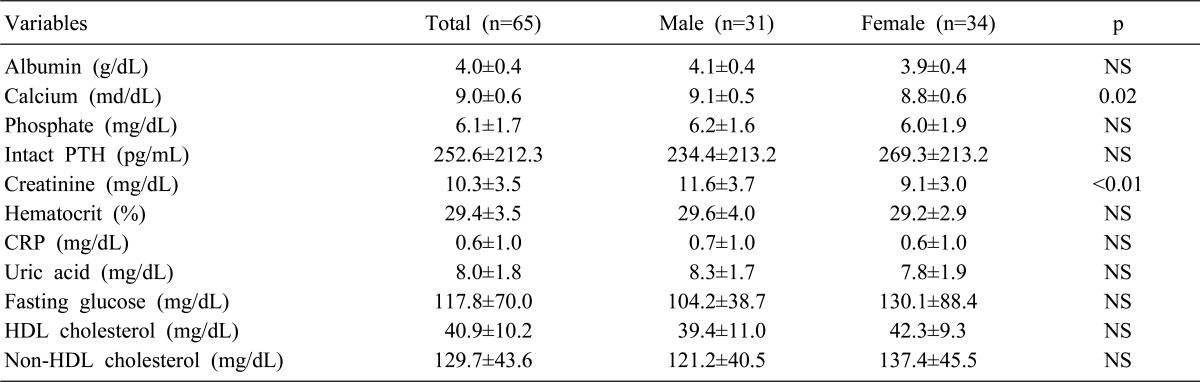
Table 2 shows the biochemical parameters. Mean serum calcium was 9.0 mg/dL and it was significantly higher in males than in females (male: 9.1 mg/dL; female: 8.8 mg/dL; p=0.02). Serum creatinine was 11.6 mg/dL and 9.1 mg/dL in the males and females (p<0.01). Mean fasting glucose was 117.8 mg/dL, which was higher in females than in males but didn't have statistic significance (male: 104.2 mg/dL; female: 130.1 mg/dL; p=NS)
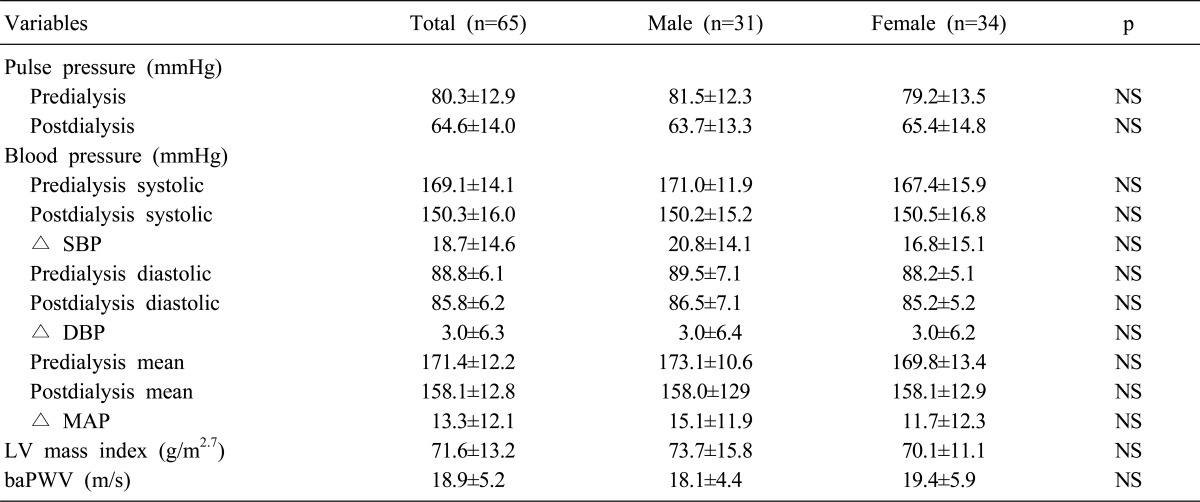
Table 3 shows cardiac parameters. Pulse pressure at predialysis and postdialysis were 80.3±12.9 mmHg and 64.6±14.0 mmHg. Predialysis and postdialysis SBP were 169.1±14.1 mmHg and 150.3±16.0 mmHg, and predialysis and postdialysis DBP were 88.8±6.1 mmHg and 85.8±6.2 mmHg. LV mass index was 71.6±13.2 g/m2.7, and baPWV was 18.9±5.2 m/s. These parameters have no significant difference between both genders.
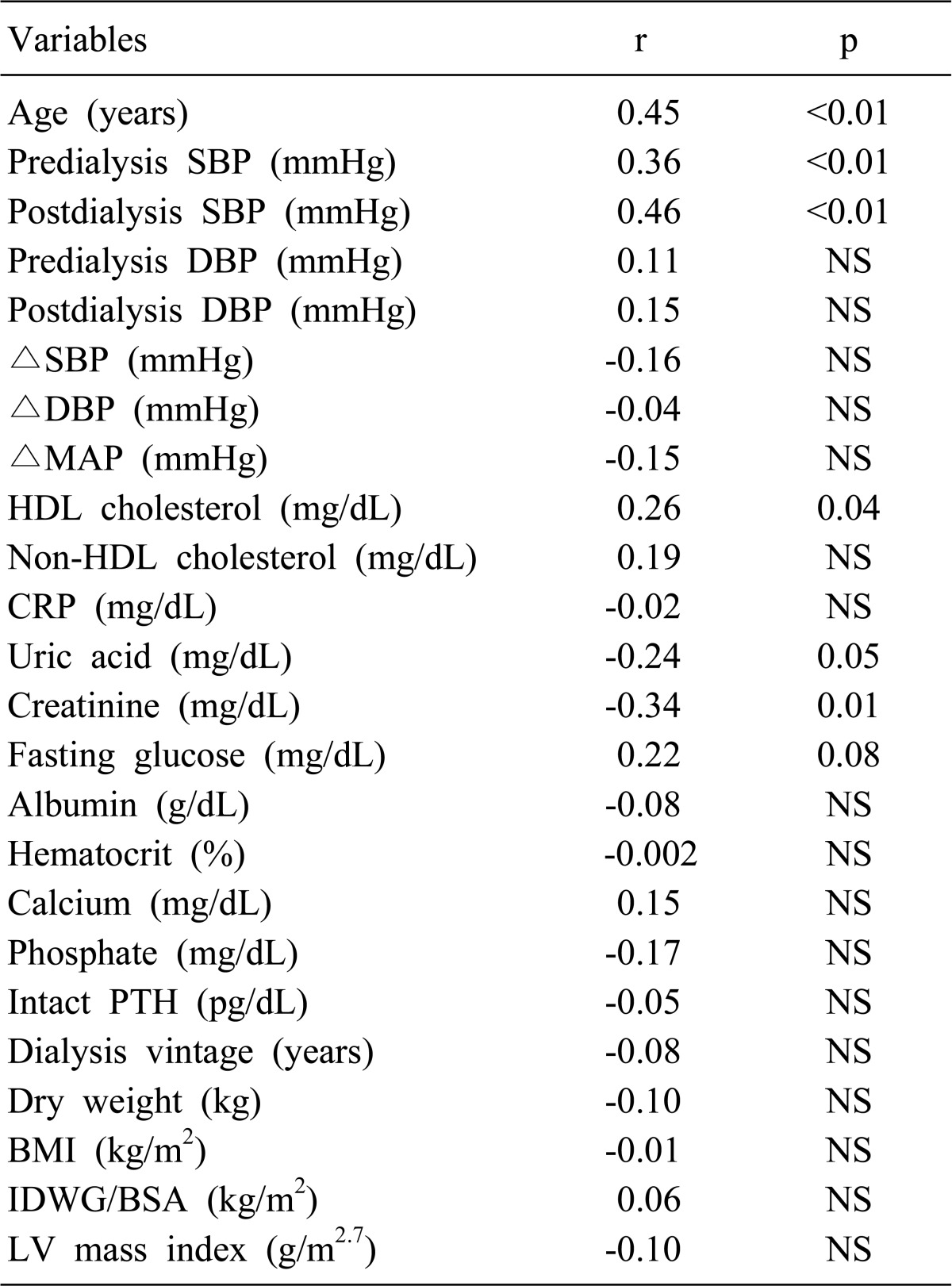
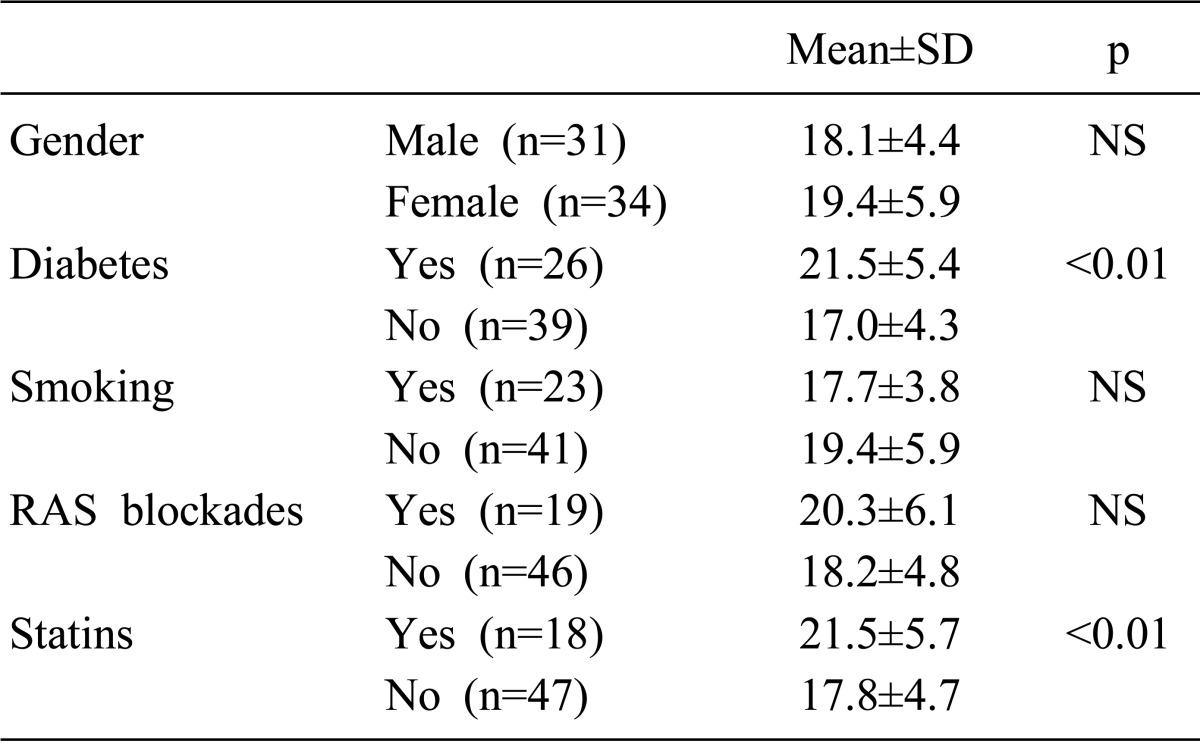
In simple regression analysis, baPWV was significantly correlated with age, predialysis SBP, postdialysis SBP, HDL cholesterol and creatinine, and marginally correlated with uric acid (Table 4). In the diabetic group, baPWV was significantly higher than in the nondiabetic group (21.5±5.4 m/s vs 17.0±4.3 m/s, p<0.01). baPWV was 21.5±5.7 m/s and 17.8±4.7 m/s in the statin group and in the nonstatin group (Table 5). There were no significant correlations in gender, smoking habits, and RAS blockades.
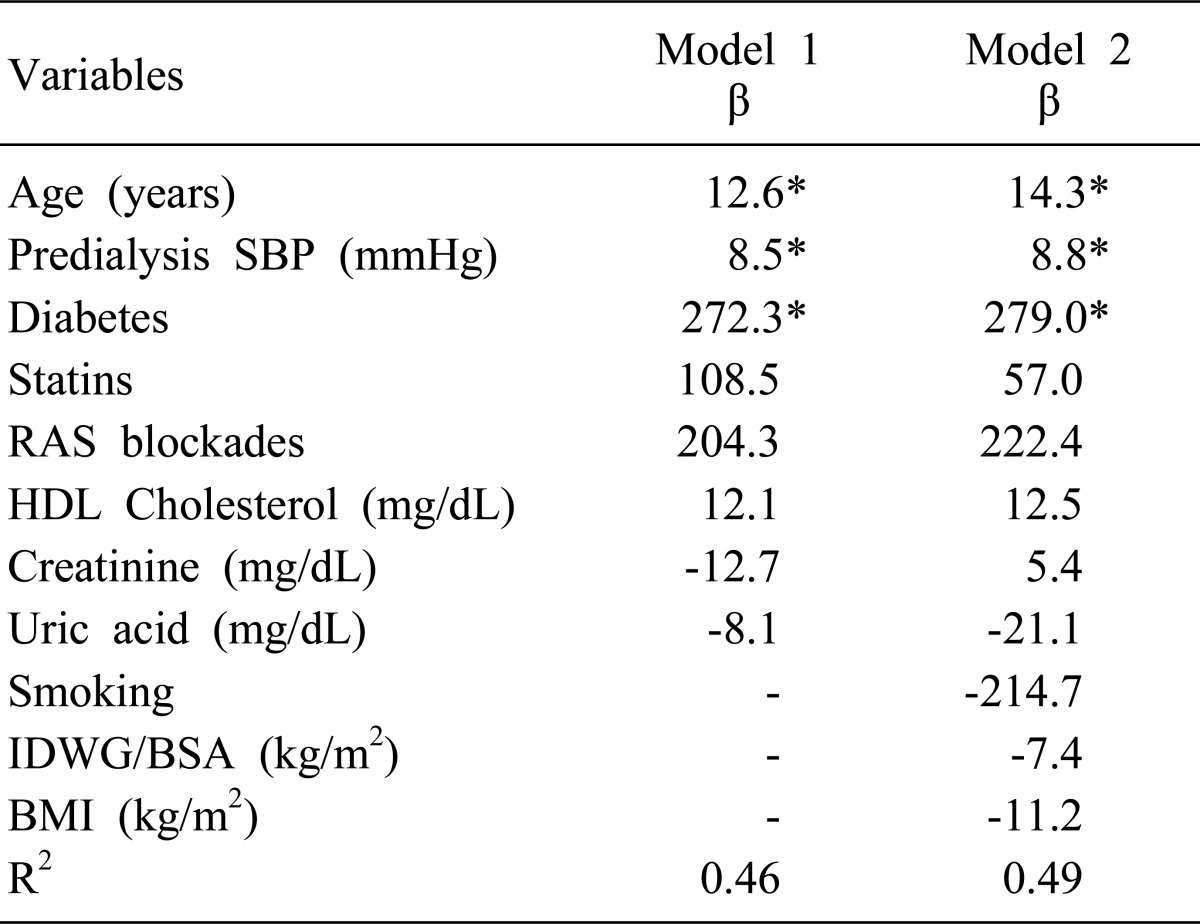
Factors associated with baPWV were evaluated by multiple regression analysis (Table 6). Increased baPWV was associated positively with age, predialysis SBP, and diabetes (model 1). In model 2, which included 11 variables, the result was similar to that of model 1.
Discussion
In ESRD patients, cardiovascular mortality is due to atherosclerosis of large arteries. Atheroma of the vessel intima causes ischemia and/or infarction downstream from the lesions and fatal cardiovascular diseases. Sclerotic change of arterial walls, that is stiffening, attributes to an increase in systolic pressure and pulse pressure and a decrease in diastolic pressure. The outcomes of these changes are an increase of LV afterload, LV hypertrophy, and a decrease in coronary blood flow3, 10).
Arterial stiffness has been measured as aortic stiffness using the tonometric sensor on the carotid and femoral arteries. Increased aortic stiffness was associated with age, hypertension, diabetes, and ESRD, and well established as independent predictor of all-cause and cardiovascular mortality in the general population as well as in ESRD patients4). CfPWV reflects aortic PWV. However this technique has low reproducibility because of technical difficulty.
On the other hand, baPWV is automatically measured by the oscillometric technique using blood pressure cuffs over arms and ankles, which is simple and reproducible as compared with the cfPWV measurement. While cfPWV assesses the stiffness of large, central arteries such as the aorta, baPWV reflects the both central and peripheral arteries. Therefore, it had been controversial whether baPWV can substitute for cfPWV in prediction of cardiovascular mortality. However, recent several studies reported that baPWV was the predictor of cardiovascular mortality in the general population as well as in ESRD patients5, 11) and associated with increasing age and blood pressure in the general population12), although a weaker predictor than ABPI in the prediction of cardiovascular mortality5).
In Korean ESRD patients on hemodialysis, few studies have investigated the factors associated with baPWV. Our study showed that baPWV was independently associated with age, systolic pressure, and diabetes, which is consistent with a previous Japanese study5). However, vascular calcification related factors such as a calcium-phosphate product and abdominal aortic calcium deposit index were also associated with baPWV in other reports5, 13). Aging induces the gradual replacement of the degenerated elastic fibers by collagenous fibers and calcification of the arterial wall. Also deterioration of endothelial function causes a decrease in nitric oxide secretion, an increase of endothelin secretion, and vascular smooth muscle growth. These changes promote arterial wall hypertrophy and stiffness and substantially increase PWV14). Tomiyama et al. reported that age is an important determinant independent of blood pressure in the healthy subject12). This association was remarkably strong in females compared with males, which suggests effect of gender on PWV. In contrast, Shoji et al. did not find any difference between both genders15) and this is similar to our present study (male 18.1±4.4 m/s vs female 19.4±5.9 m/s, p=NS).
In accordance with many previous studies, diabetes was associated with increased PWV5, 11, 15, 16). The nonenzymatic glycosylation of matrix proteins caused by chronic hyperglycemia, increased intima-media thickness, or medial calcification is considered as the pathogenesis of arterial stiffness17). When combined with hypertension, these changes are amplified. Among local hormonal mediators, angiotensin II is particularly important, as it induces hypertrophy of vascular smooth muscle cells and increases collagen production by fibroblasts, medicated by the effects of this peptide on the AT1 receptors16). Theoretically arterial stiffness can be decreased by the direct effect of hypertension itself and indirect effect through angiotensin II. Guerin et al. reported that angiotensin converting enzyme inhibitor reduced arterial stiffness and improved survival regardless of antihypertensive effect8). Uchida found that telmisartan produced a significant decrease in baPWV at 3 months after telmisartan treatment in patients with mild to moderate hypertension18). However, as shown in the present study, angiotensin converting enzyme inhibitor didn't have any association with baPWV in ESRD patients. This result suggests ESRD patients have different vascular characteristics from uncomplicated hypertensive patients.
ESRD patients are persistently exposed to oxidative stress, which causes oxidation of LDL-cholesterol and acceleration of atherosclerosis19). Statin may improve arterial distensibility by inhibition of the cholesterol oxidation and promotion of nitric oxide production20). Ichihara et al. reported that baPWV was significantly reduced by 6-month administration of fluvastatin in ESRD patients21). Contrary to their result, in simple regression analysis of this present study, baPWV was higher in the statin group than in the nonstatin group (21.5±5.7 m/s vs 17.8±4.7 m/s, p<0.01). However, when adjusted for age, systolic pressure, diabetes, HDL-cholesterol, creatinine, and uric acid, the association disappeared.
This study contains some limitations. Number of subjects may be too small for other factors, but age and blood pressure were proven to have an influence on baPWV. Also, because we didn't evaluate the hemodialysis adequacy, it may not be relevant to analyze the effect of some variables related with hemodialysis such as blood pressure, interdialytic weight gain, creatinine, calcium, and phosphorous. Finally, the equation coefficient used to calculate baPWV is based on the Japanese population, it is questionable whether we may apply the same equation to Koreans. Despite these limitations, it is meaningful that the present study suggests that baPWV measurement can be used to screen the high risk groups of cardiovascular mortality such as old age, hypertension, and diabetes.
In conclusion, the present study showed that age, systolic pressure, and diabetes were independently associated with baPWV. Although further longitudinal studies are necessary, baPWV can be applied to screen high risk patients as mentioned above and early intervention can reduce the cardiovascular mortality in ESRD patients.
 XML Download
XML Download