

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is the most common cause of hyponatremia in hospitalized patients1). This syndrome occurs in a variety of clinical settings, such as malignancies, pulmonary diseases, central nervous system disorders and medications. The most common cause of SIADH associated with malignancy is small cell carcinoma of lung2). Prostate cancer is a rare cause of this syndrome. Some cases have been reported in the literature since Sellwood and co-workers reported the first case of this syndrome in a prostate cancer patient3-8). To our best knowledge, it has not been reported in Korea. We report a case of SIADH with prostate cancer.
Case Report
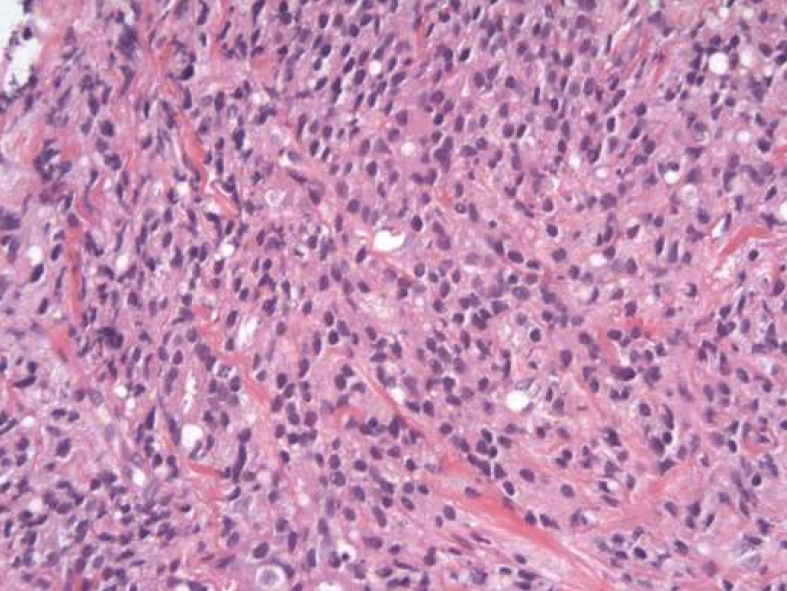
A 64-year-old male patient was admitted due to headache and nausea which had developed 1 month prior to admission. In his past history, he was diagnosed to have prostate cancer with bone metastases about 8 months ago. At that time, the pathologic finding from a transrectal needle biopsy of the prostate showed poorly differentiated adenocarcinoma, Gleason grade 5+4=9 (Fig. 1). The bone scan revealed multiple bone metastases. His serum levels of prostate specific antigen (PSA) and sodium were above 500 ng/mL and 138 mEq/L, respectively. He had received hormonal therapy, nonsteroidal antiandrogen bicalutamide in combination with gonadotropin-releasing hormone agonist goserelin. At outpatient follow up, his serum sodium level remained stable.
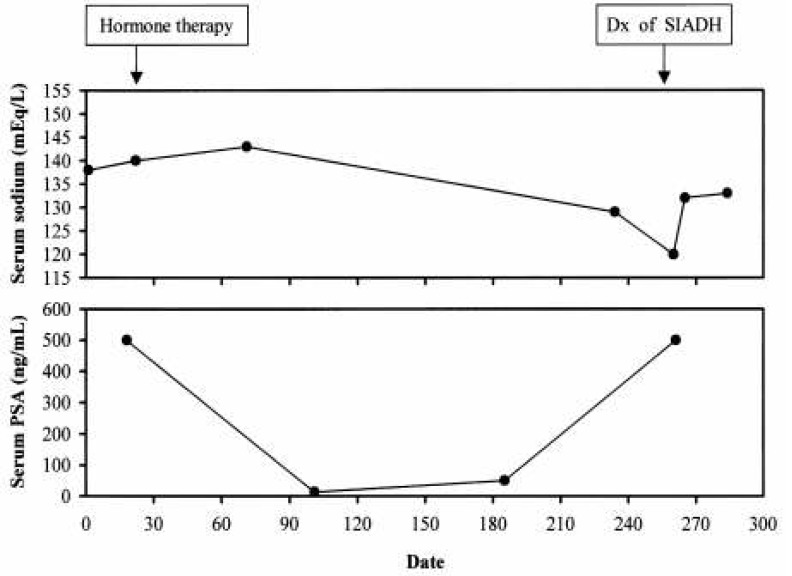
On admission, laboratory investigations showed a blood urea nitrogen level of 6.3 mg/dL; serum creatinine, 0.5 mg/dL; sodium, 120 mEq/L; potassium, 4.4 mEq/L; chloride, 86 mEq/L; glucose, 113 mg/dL; uric acid, 1.4 mg/dL; serum osmolality, 251 mOsm/kg H2O; urine osmolality, 684 mOsm/kg H2O; and plasma antidiuretic hormone (ADH), 2.5 pg/mL. The random urine sodium concentration was 223 mEq/L. The patient was clinically euvolemic. His serum PSA level was 500 ng/mL. The endocrinologic function test revealed a serum thyroid stimulating hormone level of 0.7 µIU/mL (normal range: 0.4-4.5); free T4, 1.76 ng/dL (normal range: 0.7-2.0); adrenocorticotrophic hormone, 60.3 pg/mL (normal range: 10-60); and cortisol, 22.1 µg/dL (normal range: 7-23). The Brain CT and MRI showed no abnormal findings. Cerebrospinal fluid (CSF) examination by lumbar puncture also revealed non-specific findings. Chest and abdominal CT revealed an enlarged irregular prostate and multiple osteoblastic lesions in both scapulae, ribs, vertebrae, sacrum, pelvic bone, and femoral heads, suggesting multiple bone metastases. Diagnosis of SIADH with multiple bone metastases of prostate carcinoma was made, and then correction of hyponatremia and conservative treatment were initiated. Correction of sodium concentration was achieved by fluid restriction, use of furosemide (40 mg/day) and hypertonic saline (3% sodium chloride, intravenously). Thereafter, there was greater improvement in his hyponatremia and serum sodium levels remained stable near 135 mEq/L. His symptoms also improved after correction of the hyponatremia. The clinical course of this patient is shown in Fig. 2.
Discussion
SIADH is the most common cause of hyponatremia and it results from the inappropriate release of ADH from the neurohypophysis or ectopic production of ADH. It is characterized by an inappropriately elevated serum ADH level relative to serum osmolality. Characteristic laboratory findings are hypo-osmolar hyponatremia, high urinary sodium concentration, and unimpaired renal and endocrine functions. This patient exhibited all of the serum and urinary findings consistent with this syndrome, and he was clinically euvolemic. Although his plasma ADH level was 2.5 pg/mL, this level was abnormal considering the hypo-osmolar state of this patient. In addition, diagnosis of SIADH is made by the exclusion of other causes. In this patient, all other sources of ADH secretion were excluded after extensive investigation.
The recognition of SIADH is clinically important, because hyponatremia may cause delirium, tremor, convulsions, and even coma. This syndrome may occur in a variety of clinical settings including malignancies. Of the tumors that cause SIADH, small cell carcinoma of lung is the most common, with a reported incidence of 11%2). Prostate cancer is a rare cause of this syndrome, and the pathogenesis and clinical characteristics of SIADH associated with prostate cancer have not been completely understood. Although its detailed mechanism remains unclear, it is thought that inappropriate secretion of ADH may be attributed to genetic abnormalities in tumor cells. Regarding the literature review, the majority of the reported cases presented features of an advanced stage with poorly differentiated adenocarcinoma of the prostate4-8). In addition, the prognosis of SIADH associated with prostate cancer is very poor, which is also unclear8).
In conclusion, SIADH associated with prostate cancer is a rare but potentially lethal disease. Therefore, the awareness of SIADH in patients with advanced prostate cancer would be necessary for its early diagnosis and management.
 XML Download
XML Download