

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hyperphosphatemia is a common biochemical alteration in patients with renal failure, hypoparathyroidism, pseudohypoparathyroidism, metabolic acidosis, acromegaly, and tumor lysis syndrome1). Serum phosphate is elevated occasionally in patients with multiple myeloma. However, hyperphosphatemia is rare in patients with multiple myeloma unless renal failure is present, and most cases of multiple myeloma that present with hyperphosphatemia are accompanied by significant reduction of renal function below 30 mL/min of glomerular filtration rate (GFR)2, 3). We report a case of pseudohyperphosphatemia from a patient with multiple myeloma whose serum phosphate was constantly elevated without any symptom or sign of hyperphosphatemia.
Go to : 
Case Report
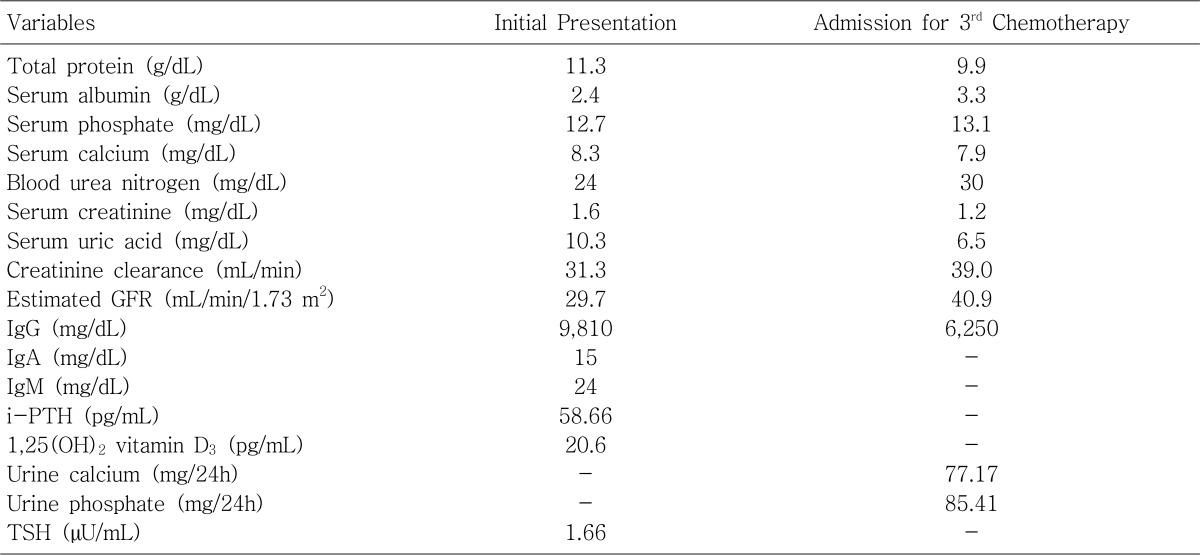
A 69-year-old woman suffered from dyspnea on exertion for a week. Severe anemia (hemoglobin 5.8 g/dL) and aortic stenoinsufficiency was revealed on her blood test and echocardiogram. She was admitted for evaluation of anemia. The albumin-globulin ratio was reversed on her blood chemistry test, and Bence-Jones proteinuria was detected by routine urinalysis. The bone marrow biopsy and serum and urine protein electrophoreses were performed, and she was diagnosed as the immunoglobulin G (IgG) kappa type of multiple myeloma. The sequential investigation showed that the stage of multiple myeloma was IIIA. There were no skin lesions such as calcified nodules or eczema, and deep tendon reflexes were normal at both upper and lower extremities. Neither lytic bone lesion nor soft tissue calcification was found on her simple radiograms. Serum creatinine was 1.6 mg/dL, and estimated GFR calculated by the abbreviated Modification of Diet in Renal Disease (MDRD) study equation4) was 29.7 mL/min/1.73 m2. Serum calcium was 8.3 mg/dL, and intact parathyroid hormone was 55.9 pg/mL. However, serum phosphate was elevated to 12.7 mg/dL. She was given mephalan 8 mg/m2 per day, prednisolone 60 mg/m2 per day for 7 days every month, and oral CaCO3 500 mg three times a day in the middle of her meal. After three months when she was admitted for her 3rd cycle of chemotherapy, serum phosphate was still elevated to 13.1 mg/dL. Serum creatinine was 1.2 mg/dL, and estimated GFR was improved to 40.9 mL/min/1.73 m2. Urinary phosphate collected for 24 hours was normal. Other laboratory findings at the initial presentation and admission for the 3rd cycle of chemotherapy are shown in Table 1.
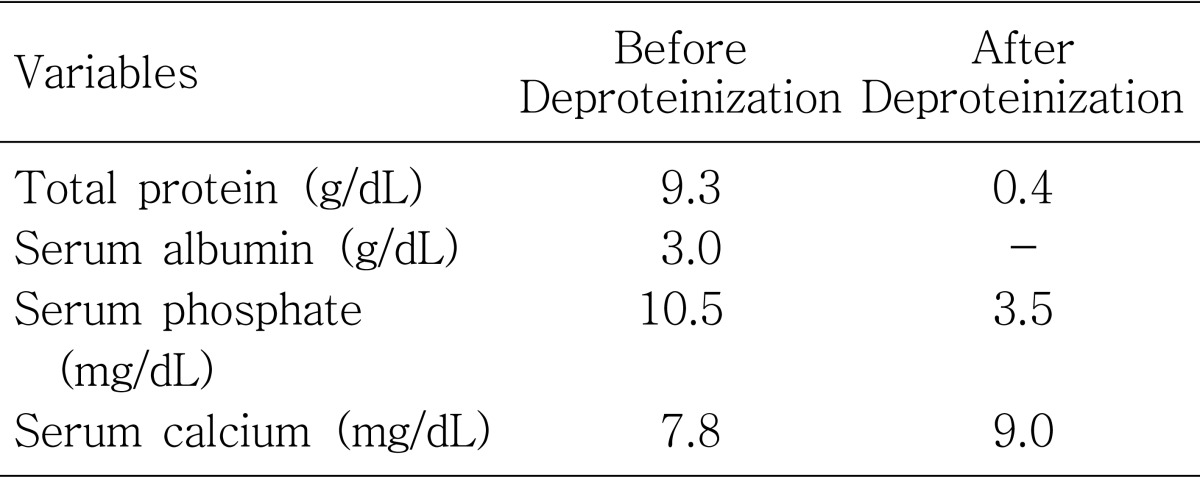
The hyperphosphatemia was suspected to be spurious because intact parathyroid hormone was normal and estimated GFR was not remarkably decreased. Therefore, we took a single blood sample from her, and split it into two. One of the samples was treated with 20% sulfosalicylate to remove the paraprotein, and the serum phosphate, calcium, and albumin concentrations were compared between the two samples. The phosphate level was decreased to 3.5 mg/dL in the deproteinized sample, but it was 10.5 mg/dL in the other (Table 2).
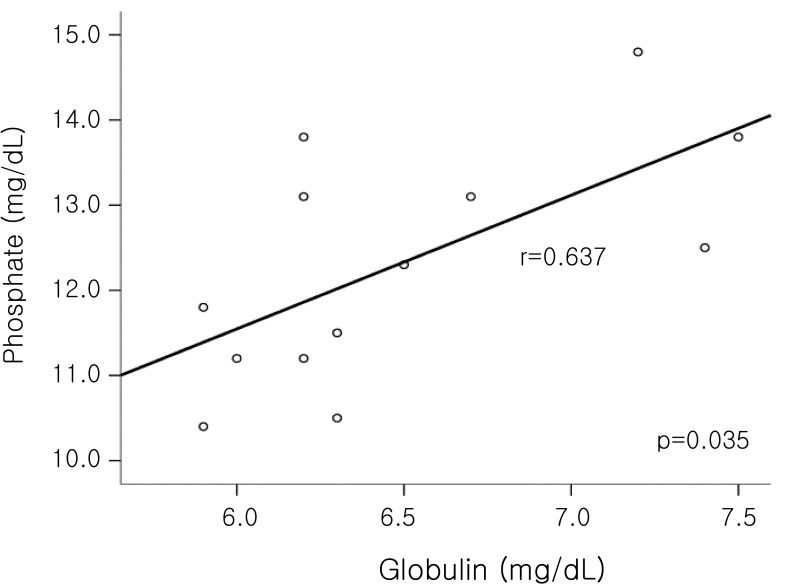
We analyzed the relationship between serum phosphate and serum globulin of the patient. Thirteen measurements were selected among all of the 21 simultaneous measurements of serum phosphate, calcium, total protein, and albumin, where the corrected calcium [= serum calcium + 0.8(4 - serum albumin)] was normal (8.2-10.5 mg/dL). Serum globulin was defined as the difference between serum protein and serum albumin. Spearman's correlation of SPSS 13.0 was used for statistic analysis. The concentration of serum phosphate was correlated positively with that of serum globulin (r=0.637, p=0.035, Fig. 1).
Finally, she was diagnosed as pseudohyperphosphatemia occurring due to the interference of serum paraprotein with phosphate measurement, and she stopped her CaCO3 medication.
Go to :
Discussion
Pseudohyperphosphatemia is characterized by falsely elevated serum phosphate due to serum paraprotein in multiple myeloma patients without impairment of renal function and clinical manifestations of hyperphosphatemia. Phosphomolybdate ultraviolet (UV) assay is most commonly used for measurement of serum phosphate5). It relies on the formation of a UV-absorbing complex between phosphate and molybdate. An inorganic phosphate reacts with an ammonium molybdate in the presence of sulphuric acid to form an ammonium phosphomolybdate complex, of which absorbance is measured at 340 nm3). Serum of a patient with multiple myeloma has falsely elevated absorbance because paraproteins react with ammonium molybdate to make the serum cloudy5-8). The level of serum phosphate returns to normal when it is measured after deproteinization with sulfosalicylate5-7, 9).
We searched the PubMed and Korean medical literature database (KMbase and KoreaMed) for similar case reports. Keyword search under "pseudohyperphosphatemia" and "multiple myeloma" was performed. Eight case reports from PubMed and 2 case reports from Korean databases were found1, 5-12) (Table 3). Han et al. reported that pseudohyperphosphatemia was identified in 6 of 67 (9%) patients with multiple myeloma8). Clinical characteristics of these cases are summarized in Table 3. Most cases were of the IgG type myeloma, stage IIIA, but other types and stages have been also reported. Existence of osteolytic lesion and serum calcium levels were inconsistent, but parathyroid hormone levels were all normal when measured. Serum creatinine levels was various, but there were no cases in which estimated GFR from the abbreviated MDRD study equation was below 30 mL/min/1.73 m2.
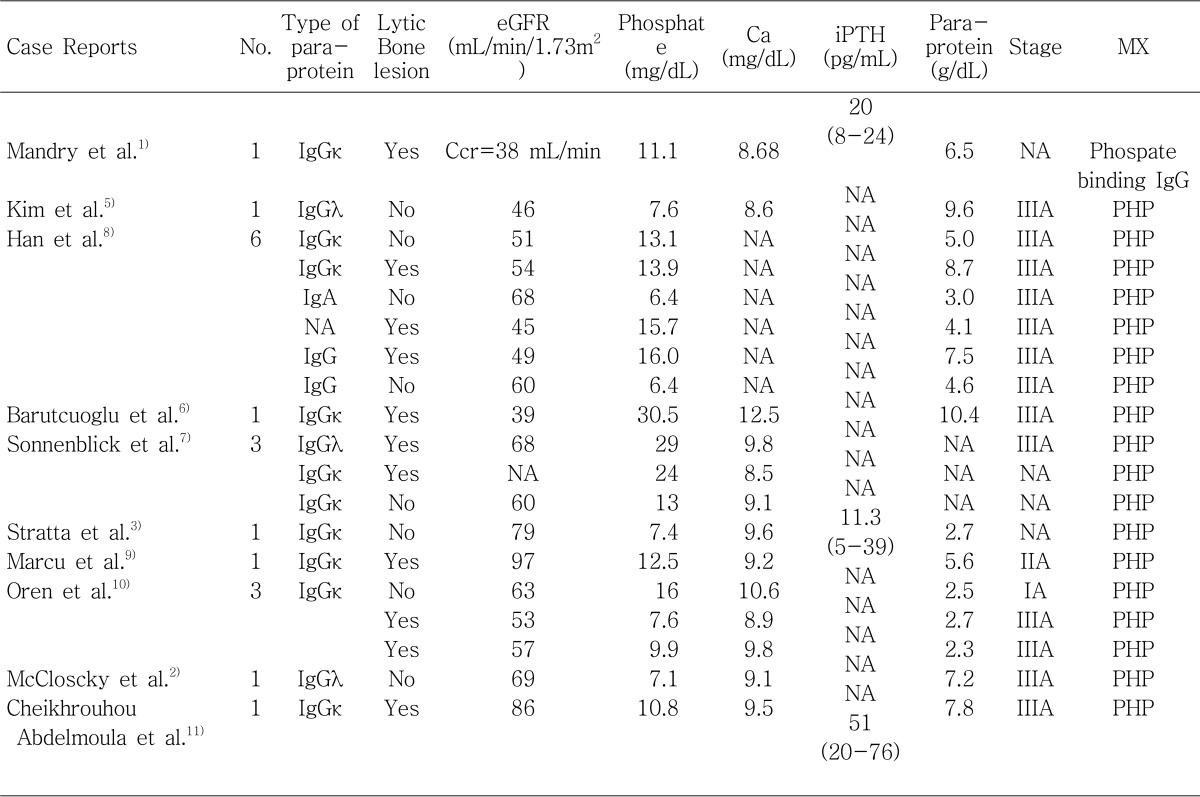
Table 3
Case Reports of Pseudohyperphosphatemia in Patients with Multiple Myeloma
No, number of case; Ccr, Creatinine clearance. Serum creatinine was not available in the paper; NA, variable that was not available in the paper; eGFR, estimated glomerular filtration rate calculated by the abbreviated Modification of Diet in Renal Disease study equation; MX, mechanism of hyperphosphatemia; PHP, pseudohyperphosphatemia; iPTH, intact parathyroid hormone; Ca, serum calcium; IgGκ, immunoglobulin G kappa; IgGλ, immunoglobulin G lambda; IgA, immunoglobulin A.
![]()
The positive correlation between serum phosphate and globulin (or immunoglobulin) has been reported in several case reports of pseudohyperphosphatemia as in ours2, 3, 5-8). It suggests that the absorbance of UV light at 340 nm increases in parallel with the concentration of immunoglobulin13). We think that the larger the tumor burden of multiple myeloma is, the greater the chances for pseudohyperphosphatemia to occur are. This could explain why the most pseudohyperphosphatemia cases were of IgG type and stage IIIA.
Interestingly, Mandry et al. reported a case of hyperphosphatemia due to phosphate-binding immunoglobulin from a patient with multiple myeloma1). The increased serum phosphate bound with immunoglobulin in the patient was demonstrated by comparison with serum phosphate in a normal control using a radioisotope method with 32P. In this case, differentiation from the pseudohyperphosphatemia was possible because hyperphosphatemia still existed when the serum was treated with sulfosalicylate because of weak phosphate binding capacity of immunoglobulin not enough to precipitate with phosphate11). Pseudohyperphosphatemia does not have any necessity of treatment. In contrast to the cases of pseudohyperphosphatemia, this case of phosphate-binding immunoglobulin had a decreased level of 1,25(OH)2 vitamin D3, suggesting a role in induction of bone diseases such as osteomalacia.
In conclusion, pseudohyperphosphatemia should be considered when serum phosphate increases in a patient with multiple myeloma whose renal function is not remarkably decreased. Analysis of the relationship between serum globulin and serum phosphate, and measurement of 1,25(OH)2 vitamin D3 and parathyroid hormone may be helpful for the identification and differentiation of hyperphosphatemia. When pseudohyperphosphatemia is suspected, measurement of serum phosphate after deproteinization with sulfosalicylate will prevent unnecessary phosphate-lowering treatments.
Go to :
 XML Download
XML Download