

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gallbladder adenocarcinoma, historically, has been considered an incurable malignancy with a dismal prognosis.12 Complete surgical resection seems to represent the only potentially effective curative treatment for resectable gallbladder cancer. Regional lymph node dissection is indispensable and invaluable for the accurate staging of gallbladder cancer.34 The extent of resection in gallbladder cancer is usually determined by the pre- and intraoperative assessment of the nature and extent of the tumor invasion. According to the National Comprehensive Cancer Network (NCCN) guidelines,5 simple cholecystectomy is considered appropriate to treat T1a gallbladder cancer. In patients with more advanced localized disease, en bloc hepatic resection and lymphadenectomy are recommended.5 Whether routine bile duct resection is medically indicated and “should be performed”, in many cases, remains a judgment call on the part of the surgeon because the surgical indication may remain unclear, even to direct inspection. There is a lack of objective evidence to support an increased long-term survival rate after routine resection, while increased morbidity has been reported.678 Several recent studies have focused on identifying prognostic factors conductive to long-term survival in those patients afflicted with advanced gallbladder cancer. Although several variables such as lymphovascular invasion, the operative method and total lymph node count of <6 have been proposed no definitive consensus has ever been achieved.3910
Current guidelines5 suggest that a selective approach to bile duct resection be implemented and utilized, with the aim of ensuring a negative margin. Despite the relative paucity of rarified, substantial medical evidence, others recommend routine bile duct resection in an effort to increase chances of disease-free survival.9 The aim of this study was to more precisely assess and identify the role of bile duct resection for T2 and T3 gallbladder cancer, vis-à-vis the specific issues of oncological and long-term survival benefit.
Go to : 
MATERIALS AND METHODS
Patients
For the purpose of this study, all patients who underwent surgical resection for documented diagnoses of gallbladder cancer at the Severance hospital, Seoul, Korea during the period January 2000 through December of 2011 were identified. Patients were included for further analysis if the pathological and surgical report confirmed T2 or T3 gallbladder cancer, and an R0 margin. The patients recruited for the study were divided into two groups: The bile duct resected (BDR group); and, the bile duct non-resected group (BDNR group). Formal comparison was made between the clinicopathologic characteristics and the follow-up data referable to the patients in each of the two groups.
Preoperative studies
All patients underwent preoperative abdominal ultrasonography and computed tomography. Endoscopic ultrasonography was used to identify and assess the degree of penetration of the focal malignancy into the gallbladder wall in patients with suspected invasive lesions. Positron emission tomography was performed to evaluate distant metastases after laparoscopic or open cholecystectomy in patients with incidentally-diagnosed gallbladder cancer. Blood levels of carbohydrate antigen 19-9 (CA 19-9) were evaluated as a tumor marker. The medical history of each participant patient was scrutinized, and all patients underwent physical examinations, baseline laboratory testing, electrocardiography and chest imaging.
Surgical strategy
The standard surgical procedure undertaken was radical cholecystectomy (involving cholecystectomy and segment 4b/5 liver resection around the gallbladder bed), with a margin of approximately 2 cm. However, some surgeons did not perform liver resections (in those cases where intraoperative inspection and the findings did not reveal gross liver invasion). Lymph node (LN) dissection was classified as either “D1” or “D2” dissection. The D1 was defined as “dissection around the hepatoduodenal ligament (including LN removal around the cystic duct, bile duct, portal vein, and hepatic artery) and dissection of LNs around the gastrohepatic ligament”. The D2 dissection was defined as “D1 dissection plus dissection of the celiac LNs, pancreaticoduodenal LNs, and para-aortic LNs”. Although the extent of lymph node dissection often depended on a judgement call by the individual surgeon, D1 dissection was routinely performed by all surgeons. Dissection of para-aortic lymph nodes and other nodes belonging to the N2 group were usually conducted when lymph node enlargement was observed intraoperatively. Para-aortic lymph nodes were excluded from the total lymph node count. The nature and extent of additional or combined resection was determined by tumor extent. Decision regarding bile duct resection depended on the surgeons' visual and tactile assessment in the operating room. During the study period within the institution, no consensus was achieved among the surgeons regarding the issue of “routine” bile duct resection. Due to the lack of consensus, some surgeons performed routine bile duct resection, while others opted to perform the procedures which they considered medically reasonable and necessary based upon dynamic assessment of the intraoperative findings during the actual surgery. Regardless, we also noted that complete clearance of the hepatoduodenal ligament including bile duct resection, was always performed in the patients with positive cystic duct resection margins, as well as those patients suspected to have direct invasion around the hepatoduodenal ligament as identified in preoperative imaging studies.
Perioperative and follow-up data
During surgery, operative procedures, operative time, intraoperative blood loss and transfusion requirement were carefully documented. Complications were registered according to the Clavien-Dindo Classification of Surgical Complications.11 Patients with advanced T-stage (T≥3) or lymph node metastasis (N≥1) were recommended for adjuvant chemotherapy, radiotherapy, or chemoradiation therapy. Patients were referred to medical oncologists, and each oncologist chose a different treatment regimen according to experience and preference. The adjuvant therapy was not provided if the patient declined the treatment, or if the patient's performance status was greater than two based on the Eastern Cooperative Oncology Group guidelines. CA 19-9 levels were checked as a tumor marker, and an abdominal-pelvic computed tomography scan was performed at three months postoperative. If and when tumors recurred, chemotherapy and/or radiation therapy were initiated dependent upon patient status. Local recurrence of tumors, such as the trocar site recurrence, was controlled by surgical excision. The tumor recurrences were categorized as “local recurrences” or “distant metastases”. The documented date of the last follow-up was set at January 2015.
Statistical analysis
For each quantitative variable, the Shapiro-Wilk test was used as a test of normality. Continual data were compared using Student's t-test or Mann-Whitney U test, as appropriate. Categorical variables were compared using the Chi-square test or Fisher's exact test, as appropriate. Survival curves were calculated by the Kaplan-Meier method; differences in the survival curves were compared by the log-rank test. Multivariate analysis identified prognostic factors of survival using the Cox proportional hazard model. Statistical analyses were performed with Statistical Package for the Social Sciences v.20 software (IBM-SPSS Inc., Chicago, IL USA). Statistical significance was defined by p-values <0.05.
Go to :
RESULTS
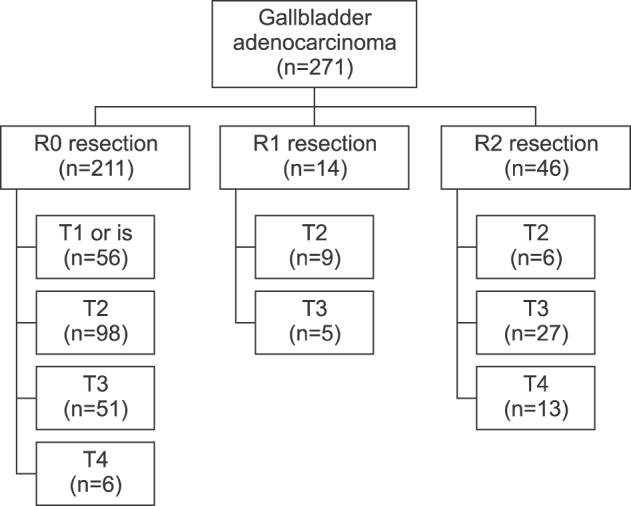
Of the 271 patients who underwent surgery for gallbladder cancer within the study period, 211 (78%) patients underwent R0 resection. Of these 211 patients, 149 (55%) had T2 or T3 disease confirmed pathologically and were included for further analysis (Fig. 1).
Clinicopathologic characteristics of patients divided into BDR group and BDNR group are summarized in Table 1. Eighty-nine patients (60%) received liver resection; of these subjects, 73 (49%) received partial or complete resection of segment 4b/5. Trisectionectomy was performed in eight patients (5%), central bisectionectomy in three patients (2%) and hemihepatectomy in five patients (3%). Combined resection of adjacent organs was performed in six patients (4%) of BDR group and included the pancreas (n=3), duodenum (n=1), and colon (n=2) (Fig. 2). Of the 50 patients with T3 tumors, invasion into the liver (n=30), serosa (n=17) and bile duct (n=3) were diagnoseded and documented.
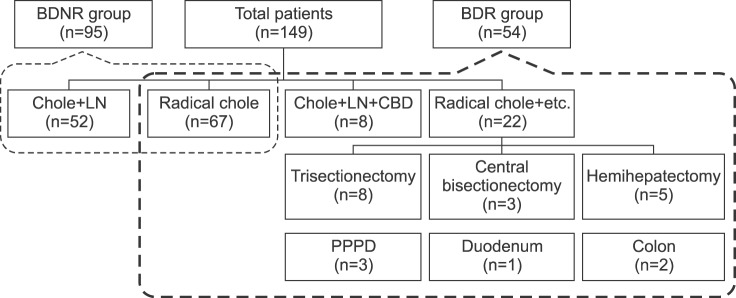 | Fig. 2Type of operative procedures. BDNR group, bile duct non-resection group; BDR group, bile duct resection group; Chole, cholecystectomy; LN, lymph node dissection; CBD, common bile duct resection; Radical chole+etc., Radical cholecystectomy and combined resection; PPPD, Pylorus-preserving pancreaticoduodenectomy.
|
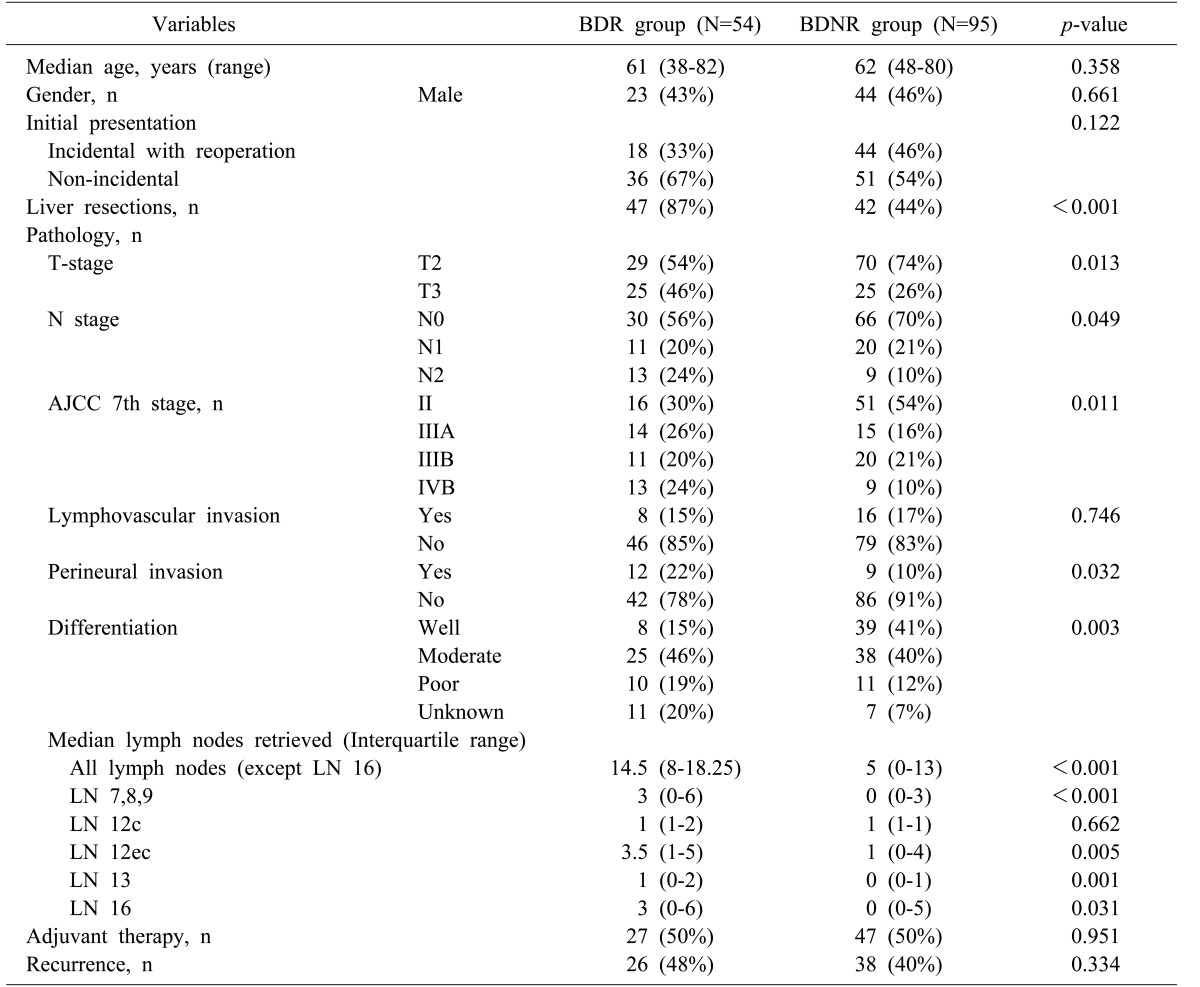
Table 1
Clinicopathologic characteristics
BDR group, bile duct resection group; BDNR group, bile duct non-resection group; LN 16, para-aortic lymph nodes; LN 7,8,9, lymph nodes around the gastrohepatic ligament; LN12c, pericholecystic lymph nodes; LN 12ec, lymph nodes around the hepatoduodenal ligament, excluding pericholecystic nodes; LN 13, retropancreatic lymph nodes
![]()
The median follow-up period for BDR group was 50 months (range: 0–145 months) and for BDNR group was 80 months (range: 0–152 months). During the follow-up period, recurrence occurred in 64 patients (43%). Local recurrences (n=8) occurred at the liver resection margin (n=4), hilar area (n=3) and trocar site (n=1).
Given the clinicopathologic heterogeneity (Table 1) among the two groups, a subgroup analysis was performed for those who underwent liver resection (n=89) with or without BDR (Table 2). In this subset of patients, only eleven of 47 patients underwent BDR for suspected invasion.
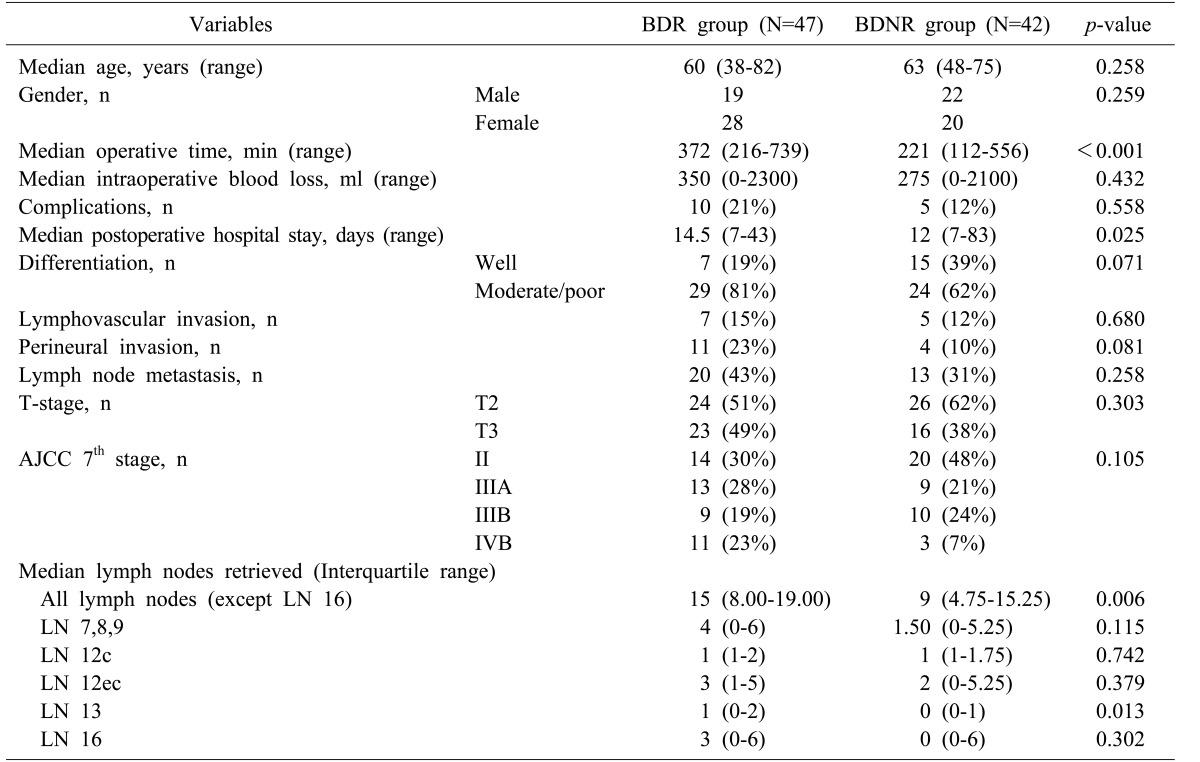
Table 2
Comparison between bile duct resection and bile duct non-resection groups for combined liver resected patients
BDR group, bile duct resection group; BDNR group, bile duct non-resection group; LN 16, para-aortic lymph nodes; LN 7,8,9, lymph nodes around the gastrohepatic ligament; LN12c, pericholecystic lymph nodes; LN 12ec, lymph nodes around the hepatoduodenal ligament, excluding pericholecystic nodes; LN 13, retropancreatic lymph nodes
![]()
While median operative time and postoperative hospital stay was significantly increased in the BDR group, complication rates were seemingly unaffected. Complications (according to Clavien-Dindo Classification) were comparable between BDR and BDNR group (p=0.558). Among 10 (21%) complications in BDR group, three were grade 1 and included ascites and seroma. One patient had a grade 2 complication with chyle drainage. Four patients had grade 3a complications and included pigtail insertions for fluid collection. Remaining two patients had grade 3b complications due to wound repair under general anesthesia.
Para-aortic lymph node (LN 16) dissection was performed more frequently in the BDR group (29 patients (62%) vs. 18 patients (43%), p=0.032).
Twenty-two patients (50%) in the BDR group and 22 patients (52%) in the BDNR group received adjuvant therapy, p=0.600.
In terms of recurrence, there was no significant difference between the two groups (21 patients (45%) in the BDR group vs. sixteen patients (38%) in the BDNR group, p=0.529. Most of the recurrences were distant metastasis.
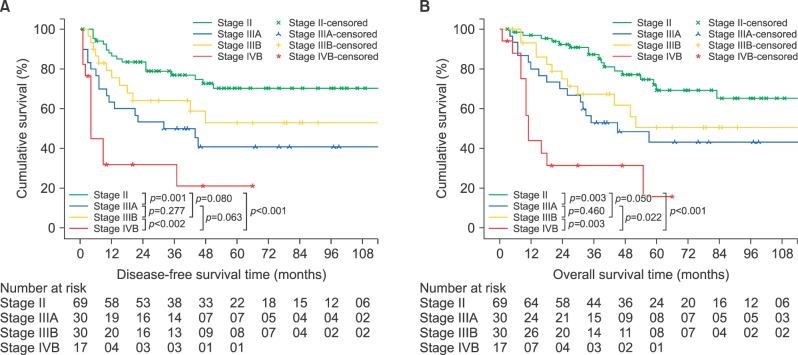
At the end of the follow-up period, 83 patients (56%) were still alive. There was a follow-up loss of three patients (2%) after the discharge from the hospital. The 5-year disease-free survival and overall survival rates were 55% and 54%, respectively. The 5-year overall survival rates of Stages II, IIIA, IIIB and IVB (according to cancer stage using the American Joint Committee on Cancer (AJCC) 7th Edition Staging) were 69%, 43%, 51%, and 16%, respectively. There were significant differences of overall survival rate according to the TNM stage, except between stage IIIA and IIIB (p=0.460). Comparisons of survival rates (according to TNM) stage are shown in Fig. 3.
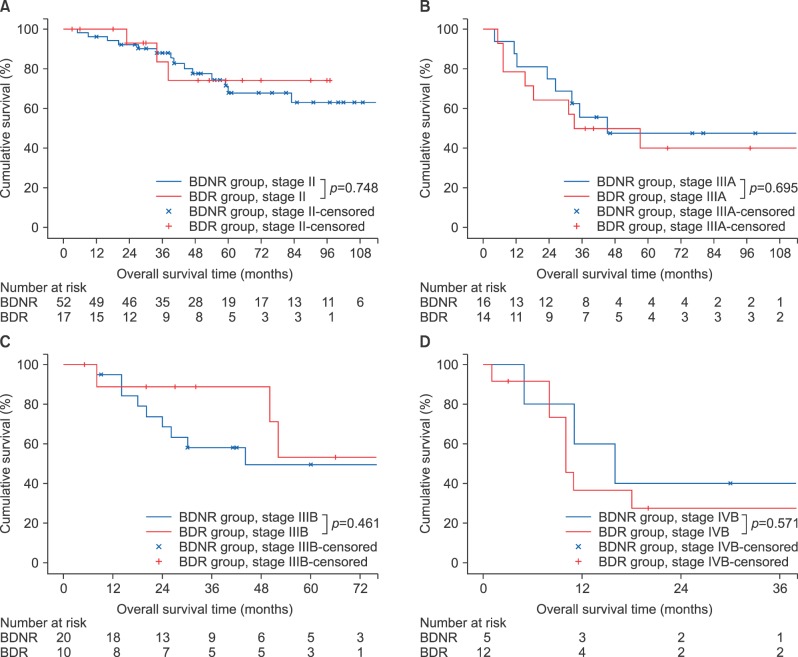
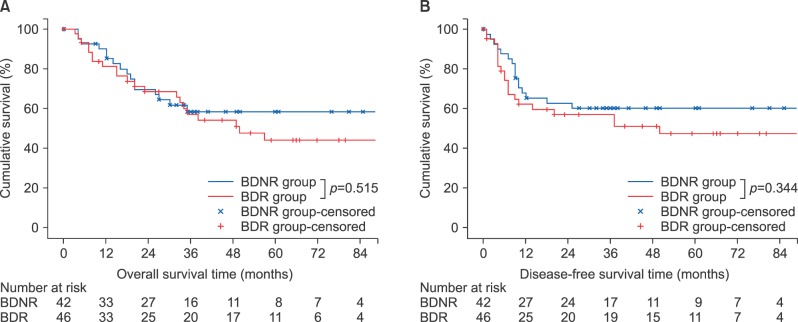
According to the survival analysis for bile duct resection, there was no evidence of survival benefit of bile duct resection in each of cancer stage (Fig. 4). Further survival analysis for liver resected patients has also shown no significant role of bile duct resection in both overall survival and disease-free survival (Fig. 5).
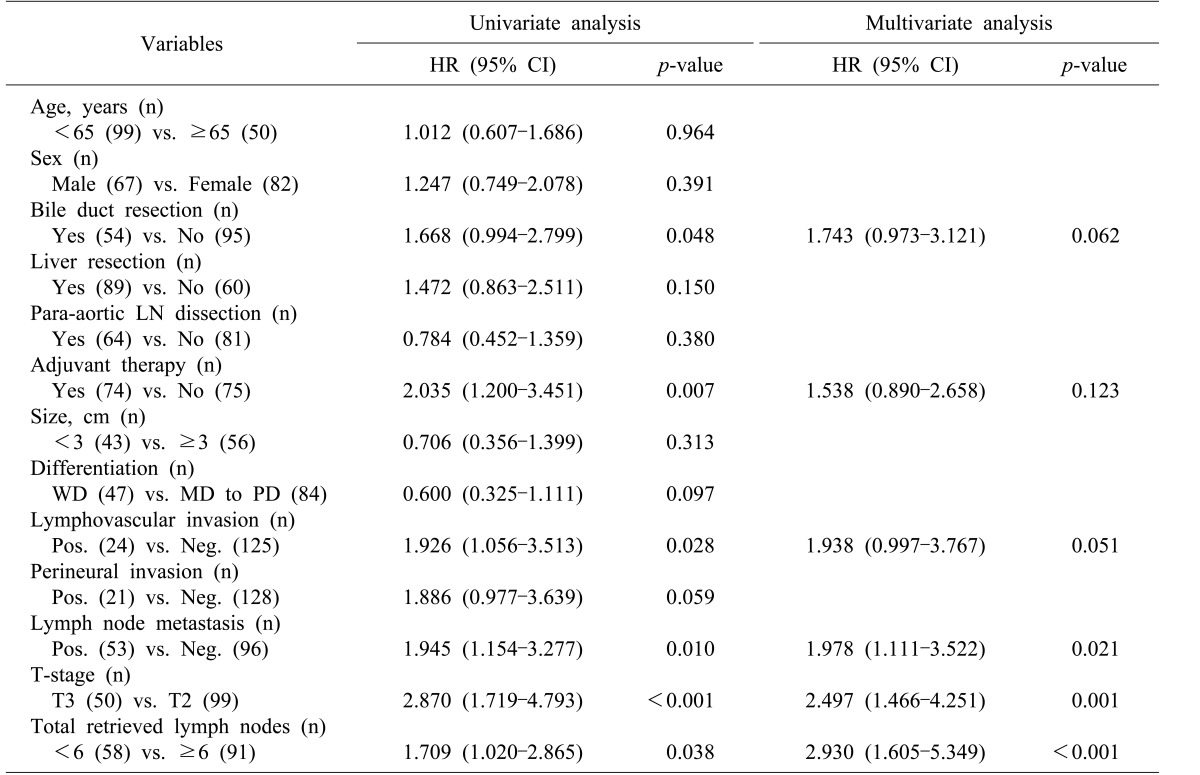
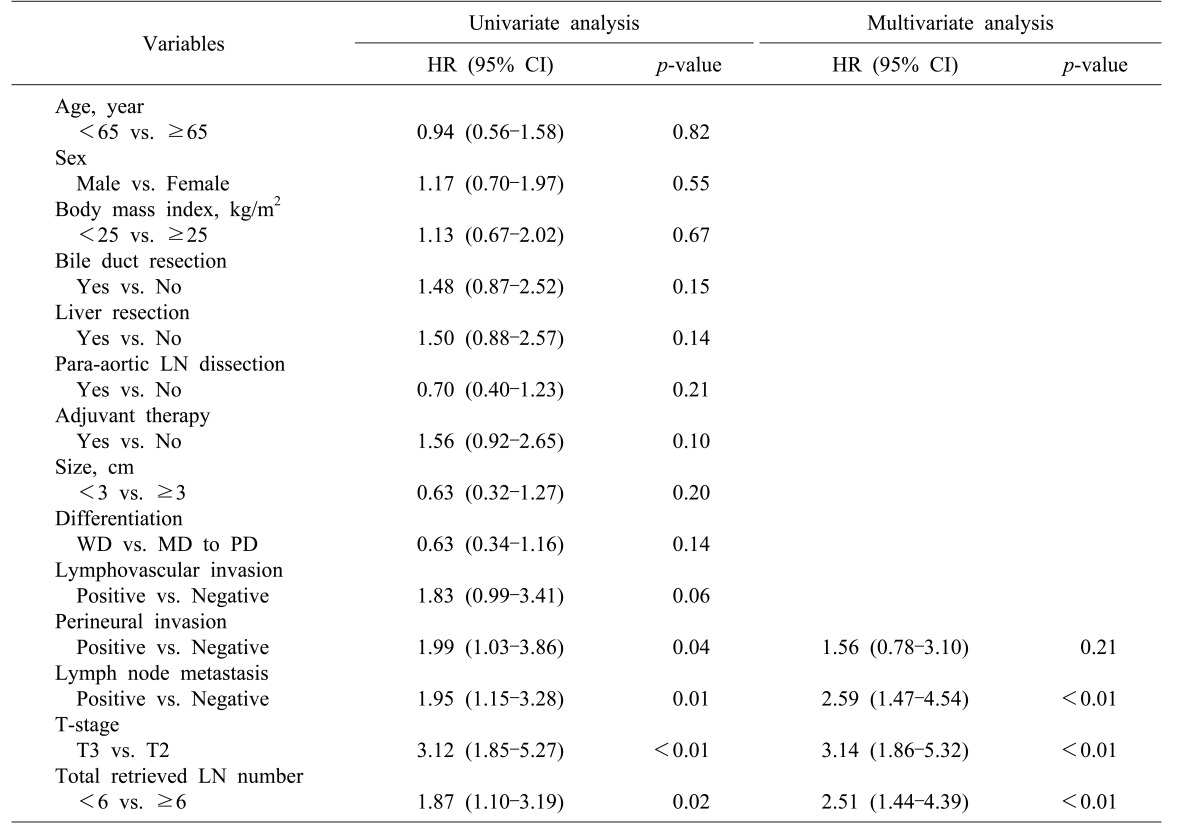
In univariate analysis for disease-free survival, bile duct resection (p=0.048) was one indicator of poor survival outcome. However, in multivariate analyses, lymph node metastasis (p=0.021), T3 stage vs. T2 stage (p=0.001), and total retrieved lymph nodes <6 vs. ≥6 (p<0.001) were the independent prognostic factors for poor survival outcome (Table 3). In multivariate analysis for overall survival, lymph node metastasis, T3 stage, and the total number of retrieved lymph nodes <6 were the independent prognostic factors of poor survival outcome (Table 4).
Go to :
DISCUSSION
The optimal extent of resection in advanced gallbladder cancer patients remains a debated issue. Chiefly, the clinical significance of concomitant bile duct resection remains controversial. Kokudo et al.7 reported no appreciable survival benefit secondary to bile duct resection in patients with LN metastasis. Sakamoto et al.8 also reported that there was no perceptible survival benefit associated with bile duct resection in patients with ≥T2 gallbladder cancer. Araida et al.6 analyzed 838 gallbladder cancer patients and reported that no survival difference resulted from bile duct resection in patients without direct infiltration of the hepatoduodenal ligament.
In the current study, there were no significant, documented differences in the overall survival between the BDR group and BDNR group, even though the BDR group patients had more advanced tumors than the BDNR group patients. Advanced T-stage, presence of LN metastasis and total LN count of <6 were the independent prognostic indicators of poor survival outcome in the multivariate analysis. In other study groups, lymphovascular invasion, perineural invasion, LN metastasis, total LN count of <6 and poor differentiation have been reported to be significant prognostic factors in patients with gallbladder cancer.3910
Adequate LN assessment is important in patients with gastrointestinal cancers,121314 because insufficient lymph node dissection during surgery impedes accurate staging. Ito et al.3 reported that the minimum LN requirement for adequate gallbladder cancer staging was six nodes. In our study, the LN count of <6 was also the prognostic factor for poor survival outcome in gallbladder cancer patients (T2 and T3 stage) who received R0 resection. The BDR group had more LNs removed than the BDNR group. Specifically, the LNs around the retropancreatic area were more frequently retrieved in the BDR group. Although bile duct resection did not affect the overall survival of gallbladder cancer patients, bile duct resection could be helpful for more accurately staging the disease.
Anatomically, the lymphatics around the hepatoduodenal ligament are the first lymphatic channels draining the gallbladder.15 Tumor cell-spread into the hepatoduodenal ligament is very frequently observed in advanced gallbladder cancer. In 2014, pathologists in Japan reported 70.6% lymphatic/venous/perineural invasion of gallbladder cancer (T2 and T3).16 In our study, the BDR group had more lymph nodes retrieved around the retropancreatic area vs. the BDNR group. While other lymph node stations did not yield more retrieved lymph nodes for the BDR group, total number of lymph nodes retrieved was significantly higher in the BDR group. These results indicate that lymph node dissection with bile duct resection allow more thorough removal of lymph nodes without leaving remnant lymph nodes and connective tissue around the hepatoduodenal ligament.
Gallbladder cancer can spread in a skipped manner. Shimizu et al.17 in pathologic analysis of 50 patients with advanced gallbladder cancer, reported that 30 (60%) patients with the hepatoduodenal ligament invasion including five patients with skipped lesion from the primary tumor. Among patients with hepatoduodenal ligament invasion, 25 (83%) patients showed cancer cells in extrahepatic bile duct and 21 (70%) patients showed occult microscopic extension. Ogura et al.18 also reported discontinuation of tumor invasion into the hepatic parenchyma. In terms of these findings, BDR has a potential benefit of eradicating occult tumor spread at the common bile duct from gallbladder cancer because of the possibility of skipped lesions not involving the cystic duct margin. We could not, however, affirm any positive effect on the long-term survival rate attributable to, or associated with, BDR. As such, it may be that the role of BDR may be limited to improved staging of gallbladder cancer as discussed in our study.
Too, the patients in the BDR group were afflicted with more aggressive cancer than the BDNR group and accordingly, surgical resection in the BDR group was also more extensive than in the BDNR group. To minimize the bias from extensive surgical resection and aggressive cancer in BDR group, only the patients with liver resection were further analyzed. Bile duct resection involved longer operative time and long postoperative hospital stays. These findings somewhat echo the findings reported by another study group.9 However, we detected no relationship between bile duct resection and the postoperative complication rate documented by our study, even though bile duct resection always required bilioenteric anastomosis. Adverse effects of bile duct resection were almost always limited to the immediate postoperative period.
Recurrence of gallbladder cancer is more likely to involve a distant site and frequently occurs in early-stage disease.1920 The peritoneum, liver and retroperitoneal lymph nodes tend to be the most common recurrence sites of a primary gallbladder cancer.20 This recurrence pattern has tended to obscure the potential beneficial effect of bile duct resection in obviating a local recurrence. Moreover, patients with advanced cancer received adjuvant therapy, which has reported favorable results with regard to the survival benefits for gallbladder cancer.2122 The recurrence rate in the BDR group was not significantly different from that of the BDNR group in this study. To estimate the relationship between the recurrence rate and bile duct resection, the effectiveness of bile duct resection for accurate lymph node dissection must be evaluated further.
About half of the patients who participated in this study received adjuvant therapy. Thirty-three patients in the BDR group and 22 patients in BDNR group belonged to 7th edition AJCC stage of greater than IIIA group. With 22 patients in each group undergoing adjuvant therapy, eleven patients in the BDR group did not receive adjuvant therapy due to patient refusal or poor performance status. This may have confounded the results in survival analysis. Moreover, results of this study may have been influenced by heterogeneous nature of the adjuvant therapy. Due to limited size of this study, further subgroup analysis on different regimens used was not possible. With more uniform adjuvant treatment, better analysis on the efficacy of bile duct resection may by possible.
Bile duct resection seems to only influence staging and no benefits on survival have been revealed from this study. Accurate staging in gallbladder cancer is still important. Lack of survival benefit in bile duct resection may be influenced by lack of uniformity in adjuvant treatment. Further evaluation of bile duct resection, with homogenous adjuvant treatment regimen, should be considered viable treatment options, for therapeutic and diagnostic purposes, and to gain further insights into survival benefits.
In conclusion, advanced T-stage, LN metastasis, and LN count <6 were the independent prognostic factors for overall survival and disease-free survival in patients with T2 and T3 gallbladder cancer. The BDR group had more lymph nodes retrieved vs. the BDNR group, and bile duct resection did not increase complication rate. The role of bile duct resection may be limited to improved staging and without affording any actual long-term survival benefit, based upon the current study. However, without any documented, significant increase in morbidity of the BDR group, bile duct resection should be actively considered as in patients with suspicious invasion around hepatoduodenal ligament.
Go to :
 XML Download
XML Download