

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
‘Situs inversus totalis’ is a rare congenital anomaly characterized by the transposition of the thoracic and abdominal viscera through the sagittal plane, resulting in a mirror image of normal anatomical structures. The disease is, generally, an autosomal recessive genetic condition, though it may be X-linked, and has also been found in identical twins with an estimated incidence of 1 per 5000-20,000 live births.1234
Anatomically, the condition is associated with the liver and gallbladder being situated on the left side of the abdomen, the stomach and spleen on the right side of the abdomen, and the heart located on the right side of the thorax. It may also be associated with several other abnormalities including bronchiectasis, sinusitis and deficient tracheo-bronchial cilia, known as Kartagener's syndrome. The presence of symptomatic cholelithiasis, in a case with situs inversus totalis, can be a diagnostic dilemma with an atypical, left, hypochondrium pain. The management of this condition also poses its own share of technical challenges for the right-handed surgeon. The mirror image of the anatomy leads to difficulties dissecting the ‘Calot's Triangle’ and hence appropriate adaptations are a necessity, both in the preoperative setting, as well as intraoperatively.5 There have been about 40 reports of open cholecystectomies and around 20 reports of laparoscopic cholecystectomies in patients with situs inversus, according to the published literature.67
Herein, we report a case of a laparoscopic cholecystectomy performed on a patient with situs inversus totalis, discussing the technical aspects and the necessary pre- and intraoperative adaptations.
CASE
A 20-year-old female presented with dyspepsia and pain in her left, upper abdomen for the past five days. The pain was insidious in onset, originated in the left hypochondrium with radiation to the left shoulder, was constant and dull aching in nature, aggravated with fatty foods, and was relieved with analgesics and antacids. There was no history of fever, jaundice, vomiting, urinary complaints, altered bowel habits or weight loss. The menstrual history of the patient was regular. She had experienced a similar episode around three months prior, which was relieved by conservative medical therapy. She did not give any history of any medical or surgical comorbidities and had no significant drug history.
The general examination of the patient was essentially normal with no signs of jaundice, fever or anemia. When examining the abdomen, there was mild tenderness from deep palpation in the left hypochondrium, with normal bowel sounds. The rest of the abdominal examination was unremarkable. Examination of the cardiovascular system revealed an apex beat in the right, 5th intercostal space in the right, mid-clavicular line.
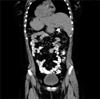
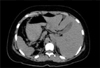
The patient's routine blood investigation revealed a normal complete blood count, normal liver and kidney function tests, normal thyroid function test and normal glycemic status. The urine examination also did not reveal any abnormalities. The ultrasonography of the abdomen showed as follows: 1) A gallbladder, small in size, with a thickened wall and situated on the left side. The lumen was filled with multiple, small calculi with posterior acoustic shadowing; 2) The liver situated on the left side, normal in size, with a homogenous parenchymal echo pattern. The intrahepatic biliary channels were not dilated; 3) The common bile duct was normal in size and diameter without any intraluminal lesions; 4) The spleen was normal in size and shape without any focal lesions and situated on the right side; and 5) Features were consistent with situs inversus. The electrocardiograph showed a right axis deviation while the chest x-ray (posteroanterior view) showed dextrocardia, the left hemidiaphragm slightly raised compared to the right side and a fundic gas shadow, of the stomach, on the right side, all findings consistent with situs inversus totalis (Fig. 1). The findings were re-confirmed with a computed tomography of the abdomen and the diagnosis was established to be a case of cholelithiasis in a patient with situs inversus totalis (Figs. 2 and 3).
After obtaining necessary anesthetic fitness, the patient was scheduled to undergo an elective laparoscopic cholecystectomy. The procedure began by adjusting the theatre equipment, including the carbon dioxide insufflator, the diathermy set and the monitor, which were placed on the left side of the patient, almost mirroring their normal positions. The patient was then positioned in the reverse Trendelenberg position after adequate anesthesia. The primary surgeon and the first assistant stood on the right side of the patient, whereas the second assistant was on the left side. A total of four ports were made - the two 10 mm ports were placed in the infraumbilical and subxiphoid regions, respectively and the two 5 mm ports were placed in the left hypochondrium in the left mid-clavicular line and in the left anterior axillary line at the level of the umbilicus (Fig. 4).
The technical challenges anticipated included creating a pneumoperitoneum from the left side, dissection of the Calot's Triangle with the right-handed surgeon using the non-dominant hand and chances of the surgeon's arms crossing during retraction of the Hartmann's pouch. The pneumoperitoneum was induced using a Veress needle through the infraumbilical incision, by the surgeon on the left side of the patient, as done conventionally. An inspection of the abdominal cavity was done and the diagnosis of situs inversus was confirmed. The camera was maneuvered from the infraumbilical port by the first assistant and the fundus of the gallbladder was retracted by the second assistant, with a toothed grasper, from the 5 mm port in the left, anterior axillary line. In order to prevent the primary surgeon from crossing arms while retracting the Hartmann's pouch from the right side of the patient, the assistant retracted it from the left side. This not only prevented the primary surgeon from crossing arms, but also enabled him to dissect the Calot's Triangle with his right hand using Maryland dissecting forceps inserted through the subxiphoid/epigastric port. The cystic duct and artery were identified and dissected free from the surrounding structures. They were clipped using titanium clips, the applicator being introduced through the 10 mm epigastric port. The gall bladder was dissected from the gall bladder fossa using a hook diathermy and was delivered outside through the epigastric port. Adequate hemostasis was ensured and the port sites were closed with non-absorbable sutures (Fig. 5).
The estimated operating time was around 70 minutes and the postoperative period was uneventful. She was discharged on the second postoperative day and the sutures were removed on the seventh postoperative day, in the outpatient department. She followed up one month after surgery and was found to have recovered well. She has not developed any postoperative complications to date.
DISCUSSION
Situs inversus totalis is an uncommon condition with prevalence rates varying from 0.04 to 0.30%.8 Situs inversus, in itself, does not predispose to the formation of gall stones.9 However, a strong index of clinical suspicion, along with imaging modalities such as ultrasonography and computed tomography scans, are needed for the accurate diagnosis of this condition.
The first successful laparoscopic cholecystectomy in a patient with situs inversus was performed in 1991 by Campos and Sipes.10 In the following years, there have been several case reports describing this rare and technically challenging procedure. Moirangthem et al.11 reported a similar case in which the primary surgeon performed the retraction, as well as the dissection, standing on the right of the patient. We believe that in such rare and technically difficult cases, it would be easier if the retraction was done by an assistant, thereby enabling the primary surgeon to perform the dissection much more meticulously. In a similar report, Arya et al.12 performed the operation using a mirror image placement of the ports and the instruments. The primary surgeon performed the dissection, while the first assistant retracted the Hartmann's pouch throughout the surgery. In our opinion, since the first assistant performed the retraction and held the camera, this could be simplified by allowing the second assistant to retract the Hartmann's pouch, as reported in our case.
There have also been reports in the literature of this procedure being performed with modifications such as the surgeon standing in between the abducted legs of the patient (Lloyd-Davis position) as described by Yaghan et al.3 The contralateral disposition of the abdominal viscera, resulting in mirror image anatomy, poses a major technical challenge for the right-handed surgeon, who would now need to perform major steps of the procedure with his non-dominant hand. There was also a concern about the surgeon's arms crossing during retraction of the Hartmann's pouch. We adapted to these challenges by allowing the assistant to retract the Hartmann's pouch, thus enabling the primary surgeon to perform the dissection of the Calot's Triangle, as well as the clip application, using his dominant hand via the epigastric port, with adequate precision, similar to that in a conventional laparoscopic cholecystectomy. Similarly, the port placements, as well as the position of the surgical team, were also an exact mirror image of the conventional procedure. We therefore believe, that through these subtle modifications, the right-handed surgeon can perform this technically challenging procedure almost as skillfully as a left-handed surgeon, in such cases.
It may thus be concluded that a laparoscopic cholecystectomy in a patient with situs inversus is feasible and may be recommended as the procedure of choice in such cases. The procedure can be performed safely, as well as with precision, by a right-handed surgeon with meticulous preoperative planning and intraoperative adaptations, resulting in operating times comparable to conventional cases.



 XML Download
XML Download