

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A central pancreatectomy is a conservative surgical procedure that preserves the spleen and pancreatic parenchyma. It was proposed as alternative to distal/extended distal pancreatectomies.12 The advantage of a central pancreatectomy is better preservation of both endocrine and exocrine pancreatic function, compared with a distal pancreatectomy,2 an extended distal pancreatectomy,3 and a spleen-preserving distal pancreatectomy.4 The major drawbacks of a central pancreatectomy are high morbidity and non-nil mortality rates,156 particularly in aged and obese patients with diabetes.7 Pancreatic fistulae represent the main source of morbidity after a central pancreatectomy, being reported in up to 63% of the patients.1
The majority of the reported central pancreatectomies worldwide were performed for a benign/low-grade malignant tumor of the mid-portion of the pancreas.12 Thus, cystadenomas and pancreatic neuroendocrine tumors were the main indications for a central pancreatectomy.12 However, the role of a central pancreatectomy for pancreatic malignancies, such as pancreatic metastases of other neoplasms, is poorly investigated.
The aim of the present study is to assess the oncological safety of central pancreatectomies for pancreatic metastases of other neoplasms, based on data reported in the literature.
MATERIALS AND METHODS
Patients
Patients were extracted from articles identified by electronic searching in PubMed-Medline and Google Scholar and by reviewing the references of the identified articles. The searched words were “central pancreatectomy”, “medial pancreatectomy”, “median pancreatectomy”, “meso-pancreatectomy”, “middle pancreatectomy”, “segmental resection of the pancreas”, “middle segmental resection of the pancreas”, “intermediate pancreatectomy”, and “isthmectomy”. No language restrictions were made. The available survival data of patients with a central pancreatectomy for metastases of other neoplasms were extracted. The study was approved by the Ethics Committee at our institution.
RESULT
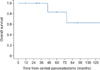
A total number of 16 patients with central pancreatectomies for pancreatic metastases of other neoplasms were identified worldwide,368910111213141516 as shown in Table 1. Renal carcinoma was the primary origin for the largest number of patients (11 patients - 69%). The mean overall survival time of the patients was 109 months, with 1-, 5- and 10-year survival rates of 100%, 84%, and 60%, respectively (Fig. 1).
DISCUSSION
Isolated pancreatic metastases of other neoplasms represent an uncommon pathology and accounts for 2%-5% of all pancreatic malignancies.1718 Thus, the reported series includes a relatively small number of patients;18192021 with most of the patients having had a renal carcinoma as the primary tumor,171821 as was the case in the present cohort of patients. Furthermore, pancreatic metastases of other neoplasms represent only 0.01%-1.8% of the indications for pancreatic resections.2223
Given the rarity of such pathology, an evidence-based surgical approach is not available. Standard pancreatic resections (i.e., pancreaticoduodenectomy, distal spleno-pancreatectomy, total pancreatectomy) are the common approaches for patients with a resectable disease.171821 However, it is not clear if pancreatic metastases of other neoplasms should share the same oncological principles as ductal adenocarcinoma of the pancreas. Negative resection margins can be achieved in some patients with central pancreatectomies for pancreatic metastases of other neoplasms but a standard lymph node dissection cannot be accomplished with this conservative surgical procedure.
The role of a systematic, loco-regional lymph node dissection for pancreatic metastases of other neoplasms remains controversial. Some studies did not find any survival differences between the standard pancreatic resections and atypical pancreatectomies for pancreatic metastases of other neoplasms and, thus, these studies do not support the routine use of systematic, loco-regional lymph node dissection.222425 However, there is a study showing that atypical pancreatic resections are associated with high recurrence rates.26 Nevertheless, there are also studies that identified metastatic lymph nodes in patients with standard pancreatectomies for isolated pancreatic metastases of other neoplasms in up to 35% of the cases.202227
After standard pancreatic resections for isolated pancreatic metastases of other neoplasms the reported median/mean survival time varied between 19 to 119 months, with 5-year survival rates between 36.2% and 88%.171819202123 These results are comparable with those reported in the present study. Consequently, a central pancreatectomy appears to have similar oncological outcomes to standard pancreatic resections.
Pancreatic metastases of other neoplasms are widely considered to be a part of a systemic oncological disease.18 These patients are likely to receive chemotherapy. Chemotherapy in a patient with diabetes can be challenging because some chemotherapeutic agents can lead to or exacerbate potential renal, cardiac or neuropathic complications complications.28 Thus, sparing the pancreatic parenchyma represents an important issue in these patients and has the potential to mitigate the complications of chemotherapy by reducing the risk of postoperative diabetes.2124 It is widely accepted that a central pancreatectomy, of all of the pancreatic resections, has the lowest potential of developing postoperative diabetes.12 Nevertheless, corticosteroids, that are often used to prevent chemotherapy-induced nausea and vomiting, may also induce diabetes in approximately 20% of the non-diabetic patients.2829
The results of this study should be regarded with caution because there are important limitations. The study includes a small number of patients, coming from many surgical centers, with different approaches and criteria selection, for a parenchyma-sparing surgical procedure. Furthermore, the group included patients with different primary tumors, and no data are available for the adjuvant/neoadjuvant treatments. It is worth mentioning that a recent multicenter study has shown no survival benefit of pancreatectomies for isolated metastases from renal carcinoma, compared with chemotherapy with tyrosine kinase inhibitors.30
In conclusion, although rarely performed, a central pancreatectomy appears to be an oncologically safe surgical procedure in select patients with pancreatic metastases of other neoplasms of the pancreatic body and isthmus. Sparing the pancreatic parenchyma represents an important issue in patients with such pathology because they are likely to receive chemotherapy. A conservative pancreatectomy has the potential to mitigate the complications of chemotherapy by reducing the risk of postoperative diabetes, which is the lowest after a central pancreatectomy, compared with standard pancreatic resections. However, no definitive conclusions should be drawn based on the data provided in the present study due to the limited number and heterogeneity of the patients.

 XML Download
XML Download