

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although acute pancreatitis (AP) is an acute inflammation of the pancreas and affects the peripancreatic tissue and surrounding organs, the global frequency of incidence is 12-73/100000.1 In developed countries, the most common causes of AP are obstruction of gallstone in common biliary duct (38%) and alcohol intake (36%).23 Other etiologic factors can be classified as pancreatic divisum, hypercalcemia, post-ERCP (endoscopic retrograde cholangiopancreatography), idiocentric drug reactions, hypertriglyceridemia, trauma, infections, hereditary, abdominal trauma, ischemia, autoimmunity, and idiopathy.4 In the current study, we have classified AP as acute biliary pancreatitis (ABP) and acute nonbiliary pancreatitis (ANBP), based on their etiologies.
Sudden onset of epigastric pain, increase of serum amylase and lipase values more than three times, and the ultrasonography (USG), computed tomography (CT) and magnetic resonance imaging (MRI) findings of at least two pancreatic indications mentioned previously, are required for the diagnosis of AP.56 According to the revised Atalanta classification wherein the edematous and necrotizing forms are clinically separated, the disease is grouped as mild, moderate or severe. While the incidence of severe pancreatitis is 20%, the mortality rate of patients is only 5%. The mortality rate increases with infected necrotic conditions. While organ damage and local complications are rarely seen in mild pancreatitis patients, they are more frequently encountered in moderate pancreatitis.67 In AP pathophysiology, the most widely observed indication is a local/systemic inflammatory response due to premature trypsin activity leading to autodigestion in the pancreatic tissue.8 No complete consensus has been reached in the pathophysiology and proinflammatory factors examined.910 The chemokine IL-8 was evaluated in the development and severity of the inflammatory response. Chemokines are divided into four subfamilies, depending on the presence of four cysteine residues in conserved locations of the primary structure, and whether the two amino terminal cysteine residues are adjacent or separated by one other amino acid. Four subfamilies are CXC, CC, C and CX3C. To date, IL-8 mainly belongs to the CXC subgroup.11 However, many researches have shown differing results due to heterogeneity. Studies have determined that IL-8 expression increases in ABP patients, having 100% sensitivity, 81% specificity, and 88% diagnostic accuracy in acute pancreatitis, within the first 24 hours.1213
Acute pancreatitis was diagnosed on the basis of clinical findings, laboratory and imaging findings. Although there is no gold standard diagnostic method, amylase and lipase released from the pancreatic acinar cells are the basic laboratory tests in AP diagnosis. However, C-reactive protein (CRP), which is an acute phase reactant released from hepatocytes, is one of the important indicators of inflammation. CRP increase in the early stages of pancreatic necrosis is significant in terms of being an indicator of disease severity. Other parameters such as serum alanine transaminase (ALT) and aspartate transaminase (AST) are also high; increase of bilirubin levels and rise in leukocyte levels were also investigated as clinical laboratory parameters for AP.211141516
Among the imaging modalities, the CT findings contributed majorly in determining the stage and severity of the disease. Pancreatitis heterogeneity, peripancreatic tissue and changes in the perirenal fascia thickness indicate that the affected organs and liquid assets, pancreatic necrosis findings and presence of pseudocysts, help in clinically assessing the severity of the disease.36
In this study, we investigated gallstone originated ABP and ANBP patients, and whether there was a predisposition to AP associated with IL-8 gene polymorphism, when compared to healthy population. In addition, we examined whether both groups of patients had different genetic polymorphisms according to the severity of the disease. We investigated laboratory parameters, which may be important in the diagnosis of the disease stage, according to the levels of normal serum values, and analyzed the significance in terms of the polymorphism number IL-8 rs4073 (-251T/A).
Go to : 
MATERIALS AND METHODS
Between January 2010 to September 2014, patients diagnosed with ABP and ANBP, were hospitalized at the Istanbul Medeniyet University of general surgery and gastroenterology clinic. Their consent was received for participation in genetic research; 83 patients with ABP were grouped as ABP group, and 93 patients with ANBP patients were grouped as ANBP group. Healthy adults with no history of gallstone and pancreatitis, were included into the study as the control group (CG – 100 subjects), and their informed consent for genetic contribution was similarly taken. All 3 groups were investigated and compared in terms of IL-8 genetic polymorphism.
Patients having abdominal pain, levels of amylase and lipase three times more than normal, and with gallstones identified on USG, were considered in the ABP group. Patients with a clinical history and laboratory findings of AP, but not showing gallstone in USG, were considered in the ANBP group. In addition to genetic polymorphism, laboratory tests such as white blood cell (WBC) count, CRP, ALT, AST, total bilirubin and direct bilirubin serum levels, as well as CT findings of the pancreas, were evaluated. Both patient groups were classified as mild, moderate and severe in order to evaluate genetic polymorphisms, by using revised classification of Atlanta.3 Blood samples taken from all patients were studied and compared between the groups, in terms of IL-8 genetic polymorphism. Also, implementation of ERCP, and recurrent pancreatitis development although cholecystectomy was conducted; two or more areas with fluid collection in CT, pseudocyst presence, the number of attacks were investigated in terms of polymorphisms, and the significance of difference was analyzed between the two groups. IL-8 polymorphism was investigated according to the etiologic factors detected in ANBP patients.
DNA isolation and genetic polymorphism investigation
Peripheral blood samples from patients and control groups were taken into EDTA tubes and stored at −20℃. DNA isolation from these samples was performed using the Bio Basic BS684-250 (Ontario Canada) coded commercial kit, according to the manufacturer's protocol. For IL-8 rs4073 (-251T/A) number polymorphism, the following primers were used for PCR and DNA fragment amplification - F (forward primer): 5′-CAT GAT AGC ATC TGT AAT TAA CTG, and R (reverse primer): 5′-CTC ATC TTT TCA TTA TGT CAG AG (archivesoforalbiology 5 8 (2 0 1 3) 2 1 1-2 1 7). Amplified PCR fragments were cut by the Mf II (Thermo Scientific) enzyme, and separated and analyzed in 2% agarose gel. Bands of 349 bp in homozygous TT individuals, 349+202+147 bp from the heterozygote TA individuals, and bands of 202 and 147 bp from homozygous AA individuals were obtained (Fig. 1).

Statistical methods
The SPSS 22.0 (IBM Corporation, Armonk, New York, United States) program was used for data analysis. Compliance with the normal distribution of data was evaluated by the Shapiro-Wilk test, and homogeneity of variance was evaluated by the Lenev test. While comparing the two independent groups, Independent-samples t test was used with Bootstrap results, Mann-Whitney U test was used with a Monte Carlo simulation technique. While One-Way ANOVA (Robust Testing: Brown-Forsythe) was used for comparing Multiple groups with Bootstrap results, Kruskal-Wallis H test was used with a Monte Carlo simulation technique. For comparison of categorical data, the Pearson Chi-square and Fisher exact test were evaluated with the Monte Carlo simulation technique. Quantitative data were expressed as mean±std. (standard deviation) and median Range (maximum-minimum) at tables. Categorical data were expressed with n (number) and the percentage (%). Data were examined in 95% confidence level, and p-value lesser than 0.05 was assumed significant.
Go to :
RESULT
Statistically, the IL-8 BPG rs4073 (-251T/A) number polymorphism, AA and TT homozygous alleles were significantly different between the ABP and ANBP groups, but no significant difference was obtained with regards to AT heterozygous alleles. AA, TT, and AT genotypes are additionally evaluated in terms of polymorphism, that was responsible for the susceptibility of the disease.
Group of patients with acute biliary pancreatitis
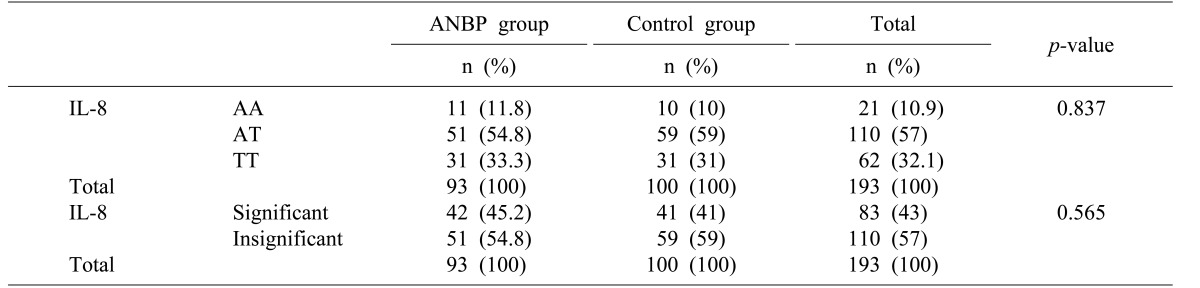
The ABP and control groups showed no statistically significant difference in terms of IL-8 rs4073 (-251T/A) polymorphism, AT, TT homozygote genotypes and alleles (Table 1). Also, no significant difference was observed between genders for IL-8 polymorphism (Table 2).
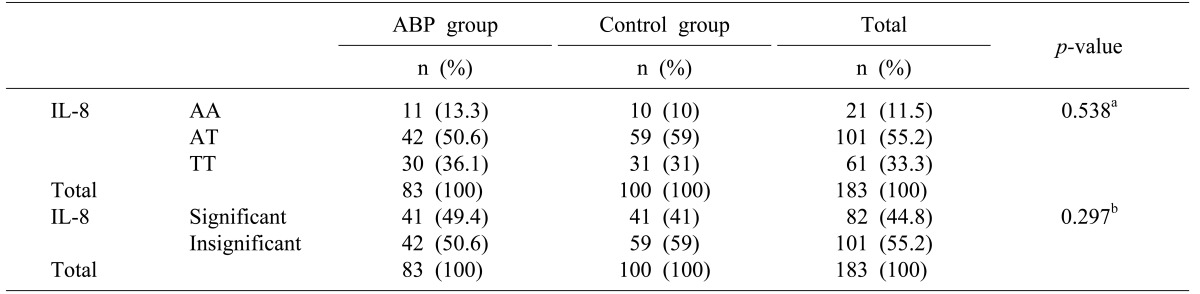
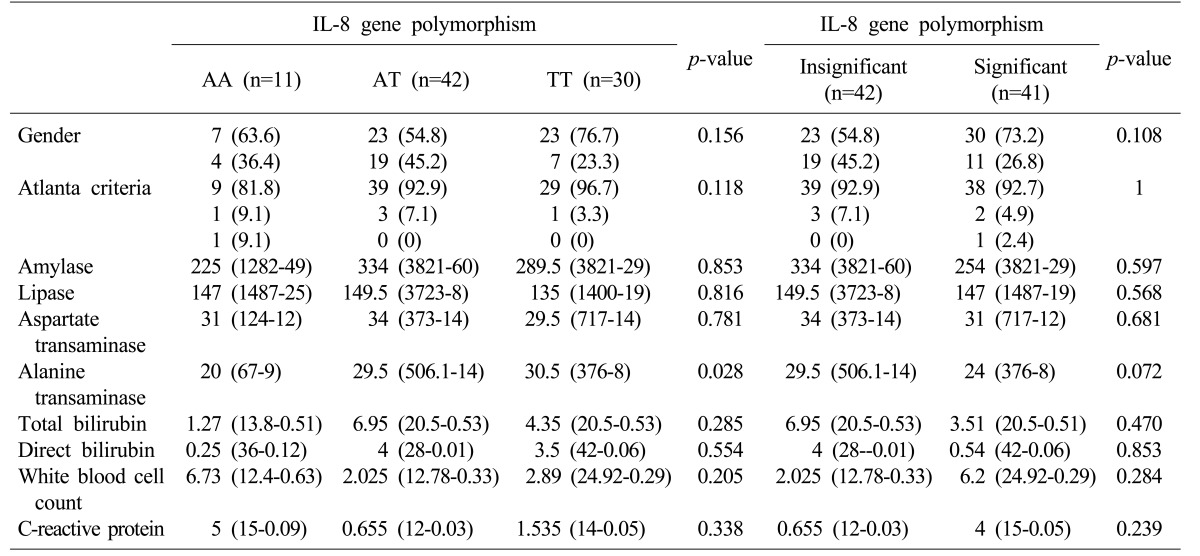
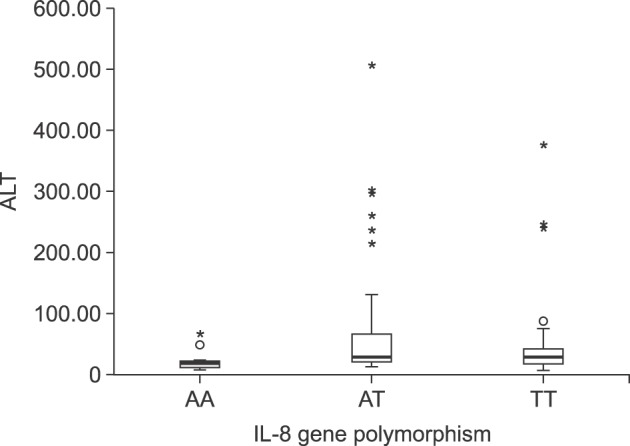
According to the revised criteria Atlanta, mild, moderate and severe pancreatitis were also not significantly different in terms of IL-8 rs4073 (-251T/A) polymorphism (Table 2). Evaluation of serum amylase, lipase, AST, ALT, total bilirubin, direct bilirubin, WBC and CRP serum levels revealed that ALT levels of patients with genotype AA were higher than in patients with genotype AT and TT (p=0.028; Table 2 and Fig. 2).
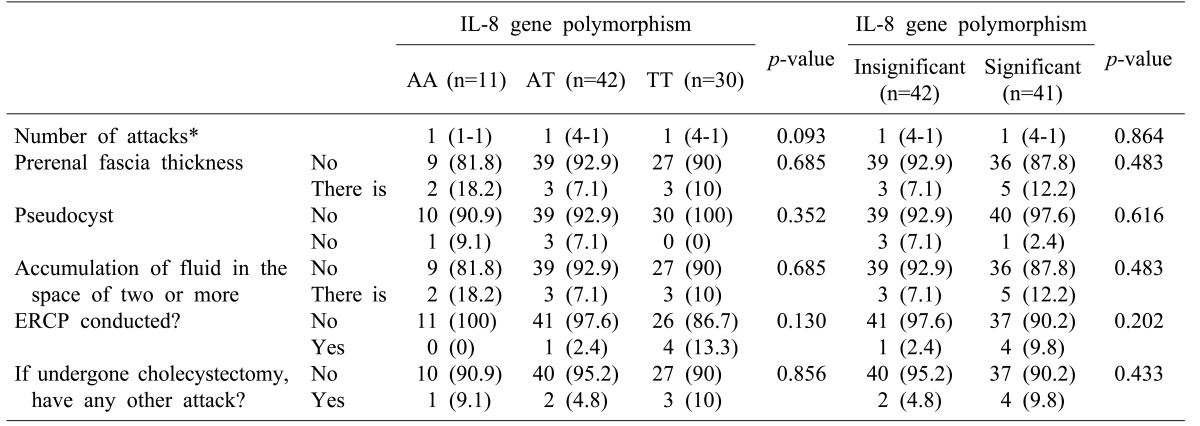
Statistical analysis revealed no significant difference between ABP group and control groups, in the following traits evaluated: the patients undergoing the disease first and more in terms of polymorphism in acute biliary pancreatitis patients (p=0.093); patients who had perirenal fascia thickness (p=0.685); fluid accumulation in two or more areas (p=0.685); presence of pseudocyst (p=0.352); the patients who had not in terms of polymorphism number IL-8 rs4073 (-251T/A) in CT findings; Further, no significant findings were observed in terms of polymorphism number of IL-8 rs4073 (-251T/A) in patients post-ERCP (p=0.130), and those undergoing recurrent pancreatitis after cholecystectomy (p=0.856) (Table 3).
Group of patients with acute nonbiliary pancreatitis
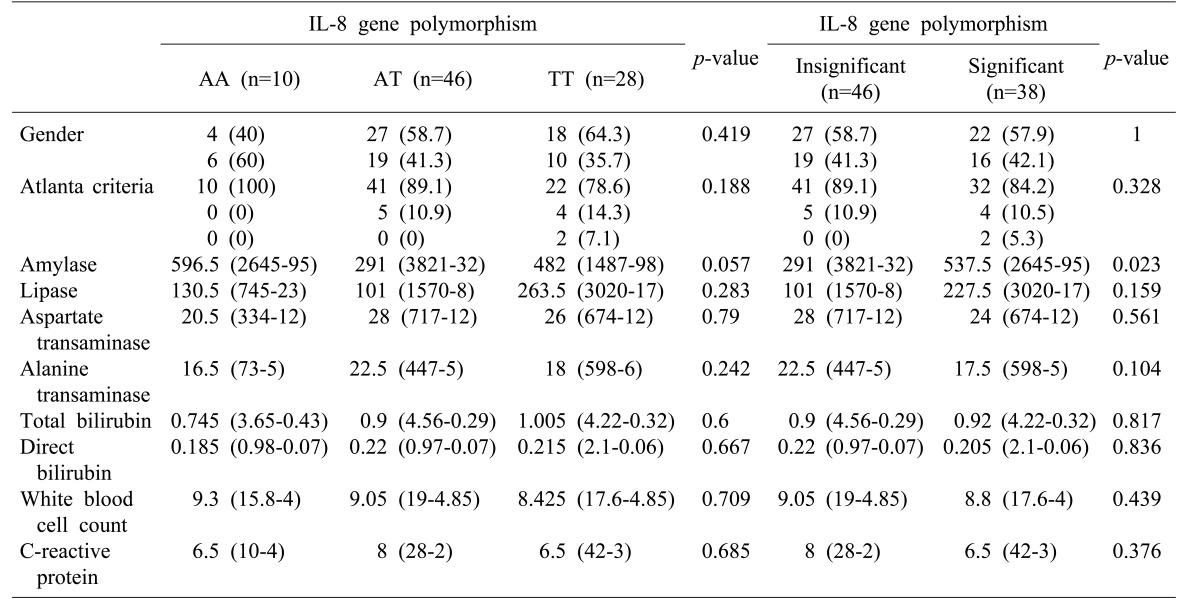
Statistical analysis between the ANBP and control groups also revealed no statistically significant difference in terms of IL-8 rs4073 (-251T/A) polymorphism, AA, AT, TT homozygote genotypes and alleles (p=0.837) (Table 4). Similarly, insignificant differences were observed between genders (p=0.419), and between mild, moderate and severe pancreatitis (p=0.188), in terms of IL-8 rs4073 (-251T/A) polymorphism according to the revised criteria Atlanta (Table 5). Evaluation of the laboratory parameters for amylase, lipase, AST, ALT, total bilirubin, direct bilirubin, WBC and CRP serum levels revealed that the increase in amylase levels was higher in patients having homozygous alleles (AA and TT) (Table 5 and Fig. 3).
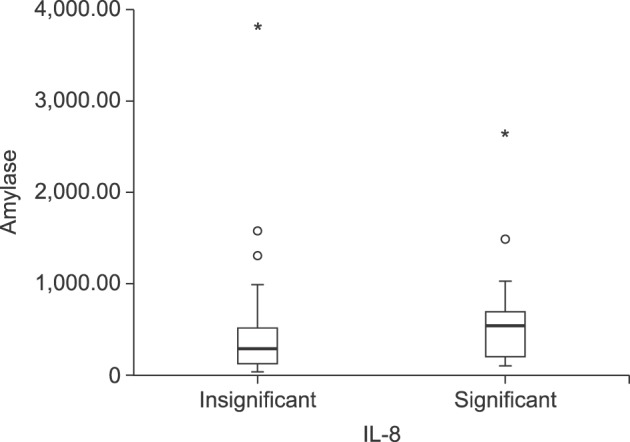 | Fig. 3IL-8 rs4073 (-251T / A) polymorphism according to amylase level in acute non-biliary pancreatitis patients.
|
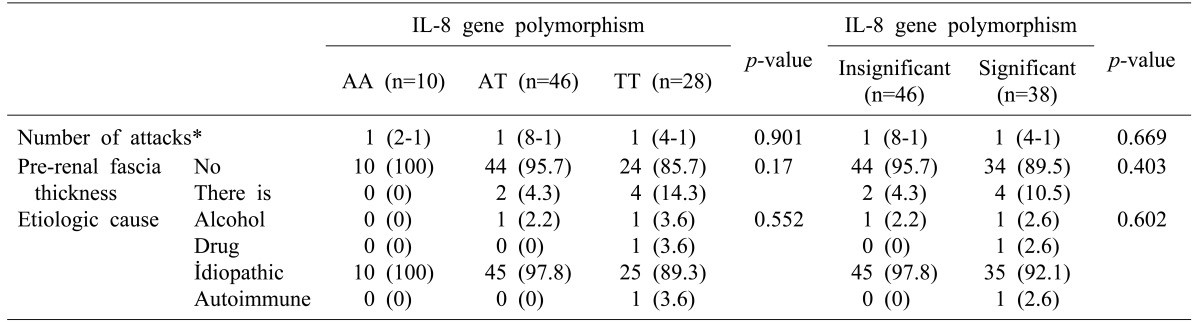
No significant differences were observed for the following traits evaluated: patients undergoing the disease first and more in terms of polymorphism in acute non-biliary pancreatitis patients (p=0.901); patients who had perirenal fascia thickness in terms of polimorphism number IL-8 rs4073 (-251T/A) (p=0.170); polymorphism between the patient groups with alcohol, drugs, autoimmune and idiopathic etiologic factors, as observed in our clinic (p=0.552) (Table 6).
Go to :
DISCUSSION
Chemokines play an important role in the onset and development of AP. In addition, due to the systemic inflammatory response syndrome which develops after onset of the disease, complications of other organs results in the development of multiple organ dysfunction.11 Being a significant activator for neutrophils, the chemokine IL-8 plays an important role in the cascade of inflammation.1718
Analyzing creation of the cytoskeleton at the cellular level, it is known that similar to other chemokines, IL-8 affects the intracellular Ca+2 changes, activation of integrins, and exocytosis of the granule protein. Like many other inflammatory diseases (psoriasis, rheumatoid arthritis, lung disease), that the levels of serum IL-8 serum are overexpressed in AP.192021 In addition, IL-8 play a key role by activating neutrophilic leukocytes in the development of acute respiratory distress syndrome, and this factor could be responsible for affecting the process in patients with severe pancreatitis.11 IL-8 is especially seen to increases in the early period of AP, and there is a correlation between the serum concentrations and the pathogenic effects formed by the disease severity.112223
Clinical studies on the rising serum levels of IL-8 in the inflammatory process have also been a lodestar for the genetic surveys, resulting in polymorphism of the chemokine, predisposing an increase towards AP.11 IL-8251 gene polymorphism was evaluated in this study. The heterozygous mutant variants in severe acute pancreatitis were frequently higher comparing with the control group (p=0.026), and the TT genotype was found higher in mild AP patients (p=0.051).11 In another study, the AA, AT and TT genotypes and alleles were examined in terms of polymorphism number IL-8 rs4073 (-251T/A). Results revealed heterozygous AT genotype in destructive AP 73.3% (p<0.05), 42.2% in edematous pancreatitis cases, and 46% in control group. No significant relationship was observed between AT genotype and destruction in AP (p<0.05).24 However, one study reported no significant difference in terms of polymorphism number IL-8 in the AP rs4073 between AP patients and healthy population. The same study also showed no significant findings in SAP.11 In our study, both ABP and ANBP patients were separately investigated for homozygous (AA and TT), AA, TT, and AT genotypes in terms of polymorphism number IL-8 rs4073 (-251T/A); no significant difference was observed when compared to control group. Also, no differences were observed in terms of polymorphism in disease severity between the two groups, according to revised Atlanta classification.
The most common etiologic causes of AP are alcohol and gallstones.825 While alcohol-related AP is more common in males, gallstone related pancreatitis is more frequent in women. The pathophysiology may be explained by the damage caused due to the obstruction that occurs in the ampulla of Vater attached to the gallstone in AP, and released stasis and fluid retention which causes the accumulation of enzymes in the pancreatic canal.26 Whatever the etiology, increase in the amylase and lipase levels are important diagnostic criteria for all APs.527 However CRP, whose serum level rises in AP, may be one of the nonspecific acute phase reactants which can be the marker of severity. The excessive leukocyte activation which develops with cytokines plays an important role in the pathogenesis of pancreatitis with inflammatory effect. Abnormal phagocytic leukocyte hyperstimulation could be the cause of fatal pancreatitis.8101528293031
Serum transaminases and bilirubin are used to identify biliary etiology from nonbiliary in AP. The increase of serum ALT level in the presence of gallstones was shown in biliary etiology, and patients with ALT>150 units/L had a positive predictive value for ABP. Serum total bilirubin value >3 mg is significant for ABP and important for identifier diagnosis.163233343536 In our study, the evaluation of laboratory parameters in patients with ABP and ANBP revealed serum ALT median value in ABP patients with AA genotype was higher than the AT and TT genotypes. No statistical significance was observed between the patients having high and normal levels of amylase, lipase, AST, total and direct bilirubin, leukocytes, and serum CRP levels (Table 4). However, in ANBP patients, the median value of serum amylase was significantly higher in patients having homozygous (AA and TT) alleles than in the AT heterozygous genotype patients. In lipase, ALT, AST, total and direct bilirubin, WBC and CRP levels, no significant polymorphism difference was observed (Table 5).
The positive predictive value for ABP when ALT values are more than three times the normal, and patients having increased ALT median values were seen most frequently in AA genotype. This could be an insight as one of the factors which increase due to the IL-8 rs4073 (-251T/A) number polymorphism. Studies conducted with larger patient population are required.
In CT findings for pancreatic growth, inflammatory changes around the pancreatic fluid collections, density changes in pancreatic tissue, and pancreatic gas formation within the intestinal tract of fistula are important diagnostic criteria for AP. At the same time, it is important for the recognition of intra-abdominal complications and the severity of the disease.3636 Balthazar classification, perirenal space and fascia signs are very important for this evaluation. According to CT accumulation of fluid in the peripancreatic area and increase in the perirenal fascia thickness, which can be evaluated as a transmission from mild to moderate form, are important findings.2373839 According to the CT findings in patients with acute biliary pancreatitis in terms of IL-8 rs4073 (-251T/A), no significant difference was observed between the patient groups who had increase in the perirenal fascia thickness and two or more areas of fluid accumulation, and those who did not have either. In the group of patients with acute non-biliary, no statistically significant finding was observed in terms of increase in perirenal fascia thickness. Correlation of the IL-8 rs4073 (-251T/A) polymorphism with CT findings in favor of disease severity was thus not observed.
However, recurrent AP pancreatitis may develop, depending on the continuance of the etiological factors. ERCP is increasingly seen to have an important place in the treatment of ABP patients with the continuation of obstruction. With removal of the obstruction, either spontaneously or after ERCP, the rate of complications was decreased in less than 48 hours, than in cases with obstructions lasting more than 48 hours. ERCP necessity can adduce continuing inflammation owing to bile duct obstruction, due to impacted stone and this condition can increase the severity of ABP. But despite sphincterotomy performed with ERCP for gallstone in the ABP patients, and cholecystectomy treatment, recurrent pancreatitis may develop due to an unknown etiology.34353640 Even though laparoscopic cholecystectomy is curative when gallbladder stones or sludge are detected, several patients who have undergone cholecystectomy present repeated attacks of pancreatitis.41 No significant difference in both groups was observed with patients having first time AP and having multiple APs. Likewise, with patients who undergone AP after cholecystectomy in ABP patients were evaluated, no statistically significant difference was observed.
Etiology is very important for the evaluation of disease severity and determination of the treatment method in patients with acute non-biliary pancreatitis. Distinguishing the alcohol-related pancreatitis from gallstone-related pancreatitis is necessary for the determination of the type of treatment. Permanent organ damage and morbidity are higher in alcohol-related pancreatitis compared to others. However, the frequency of autoimmune pancreatitis is less than 5%, and it is treatable with corticosteroids, which is different from others. In addition, autoimmune pancreatitis can be evaluated with response to steroid therapy, a method very different from the other disease manifestations. The idiopathic pancreatitis is the AP reason which may have the most serious permanent organ damage and mortality among all other etiology cases.9424344 In the present study, no statistically significant difference was observed between the alcohol, autoimmune, idiopathic and medication related ANBP patients in the evaluation carried out on the purpose of analysing whether the treatment and disease severity variables are different by etiology, and depended on the genetic polymorphism or not.
In conclusion, in our studies with patients having biliary and nonbiliary etiologies, we did not observe any statistically significant finding that polymorphism number IL-8 rs4073 (-251T/A) could form a predisposition to the disease or to its severity. However, higher ALT values determined in the genotype of the ABP, the homozygous variant (AA and TT) with high levels of amylase in ANBP patients, it should be kept in mind that this could lead to increased tissue damage in the AP patients in terms of IL-8 rs4073 (-251T/A) polymorphism.
Go to :
 XML Download
XML Download