

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
GISTs are the most common primary mesenchymal tumors originated from the gastrointestinal tract. These tumors occur mainly in the stomach (50–60%), small bowel (20-30%), large bowel (10%), and esophagus (5%).1 In rare cases, these tumors are found as primary tumors outside the GI tract, such as the omentum, mesentery, retroperitoneum, and gallbladder.23 These tumors have been designated as “extra-gastrointestinal stromal tumors” (EGISTs). EGISTs arising in the pancreas are extremely rare with limited individual case reports and small numbers of case series. Herein, we report a case of a pancreatic extra-gastrointestinal stromal tumor in a 64-year-old female patient along with a review of literature.
CASE
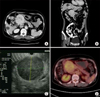
A 64-year-old woman was referred to our department for treatment of an abdominal mass incidentally detected by ultrasonographic examination during health screening in August 2010. She had no clinical symptom related to this tumor. She had no remarkable history. Physical examination revealed no specific findings. Laboratory data were within normal limits. Tumor markers were also within normal limits. Abdominal computed tomography (CT) showed a well enhanced mass measuring 6.5×6.5 cm with central low dense lesion (Fig. 1A and B). Endoscopic ultrasonography (EUS) revealed a well-defined homogenous hypoechoic mass like lesion without posterior acoustic shadowing at the pancreatic head. The main pancreatic duct was mildly dilated (Fig. 1C). EUS guided biopsy was performed, yielding pathological diagnosis of gastrointestinal stromal tumor. Positron emission tomography (PET) detected hypermetabolic lesion measured at 7 cm (SUVmax 4.0) in the pancreatic head without evidence of abnormal hypermetabolic lesion, suggesting LN or distant metastasis (Fig. 1D).
Under a preoperative diagnosis of a duodenal GIST or pancreatic neuroendocrine tumor, we performed a pylorus preserving pancreatoduodenectomy for this lesion. On pathologic gross examination, the tumor measured at 7 cm in its greatest dimension almost entirely involved the pancreatic head. It was easily separated from duodenum. Its cut surface was rubbery and white. Surrounded by a thin pseudocapsule, it was well-demarcated (Fig. 2A). Microscopically, the tumor was composed of spindle cells (Fig. 2B). Mitotic count was 5/50 high-power fields (HPF). Immunohistochemically, neoplastic cells were diffuse. They were weakly positive for antibodies against C-KIT(CD117) but positive for CD 34 and vimentin (Fig. 2C and D). However, smooth-muscle actin reactions with antibodies against S-100 or desmin were negative. Based on above findings, the tumor was finally diagnosed as EGIST originating from the pancreas.
She had an uneventful postoperative course. The patient was discharged home on postoperative day 20. Adjuvant therapy was not started due to the low mitotic rate of the tumor and its intermediate size. She is free of recurrence of EGIST after the surgery.
DISCUSSION
EGISTs arising in the pancreas are extremely rare. Reports of pancreatic EGISTs are limited to individual case reports and small number of case series. A total of 17 patients who were confirmed as pancreatic GISTs after resection were collected in this study.456789101112131415161718 The clinicopathological features and outcomes of these cases are summarized in Table 1. Age of these patients ranged from 30 to 74 years (median, 54.7 years; mean, 53.1 years). Eight patients were males and nine were females. Most clinical presentations included vague abdominal pain or discomfort, weight loss, and fatigue. However, seven (41.2%) cases were found incidentally during a workup for unrelated conditions. These tumors ranged from 6 to 35 cm in maximum diameter (median, 10.0 cm; mean, 11.9 cm). These tumors could occur in any part of the pancreas. Their most common location was head (6/17, 35.3%) and tail (6/17, 35.3%), followed by body & tail (3/17, 17.6%) and head & body (2/17, 11.8%) in the pancreas.
Characteristic immunohistochemical profile of GIST has been proven to be very helpful in its diagnosis. On immunohistochemistry, positivity of c-Kit (CD117) confirms the diagnosis of GIST. C-kit gene is expressed in 95% of cases. CD 34 is also expressed in 60-70% of GIST cases. The frequency of CD 34 positivity depends on the location of GISTs. The frequency of positive CD34 is high in GISTs of the esophagus and colon (95%). However, it is relatively low in small bowel and extra-gastrointestinal sites. GISTs may also show variable positivities for other immune markers, such as SMA (30–40%), S-100 (5%), and desmin (1–25%).19 In our review, 14 (82.4%) of 17 pancreatic EGISTs showed positivity for CD117 while 9 (52.9%) cases were positive for CD 34.
GIST exhibits a broad spectrum of clinical behaviors. The prognosis of patients with GIST depends on the biological behavior of GIST. Fletcher et al.1 have defined the criteria to estimate risks of aggressive behavior and metastasis of GIST using tumor dimension (cm) and mitotic count (/50 HPF). According to their criteria, GISTs are divided into risk categories of very low (<2 cm, <5/50 HPF), low (2–5 cm, <5/50 HPF), intermediate (<5 cm, 6–10/50 HPF or 5–10 cm, <5/50 HPF), and high risk (>5 cm, >5/50 HPF or >10 cm, any mitotic count) of metastasis.1 In our review, the risk of aggressive behavior according to Fletcher criteria was high in 13 (76.5%) cases. The remaining three (11.8%) cases had intermediate risk. The frequency of high risk aggressive behavior tended to be high for GIST.
It is well-known that resection should be considered as the first treatment choice for resectable localized GIST because high potential of malignancy is associated with cases of GIST. Complete surgical resection with negative microscopic margins is the standard treatment for GISTs.20 Systemic regional lymphadenectomy is not generally considered because lymph node metastasis is rare (prevalence of about 1%).21
Response rates of GISTs to conventional chemotherapy and radiotherapy are 10% and 5%, respectively.913 Adjuvant treatment with imatinib can be provided in order to enhance the possibility of curing the cancer by eradicating microscopic lesions that might remain after complete resection of visual tumors.19
DeMattero et al.22 have reported that most recurrence of GIST will occur within 24 months after resection, with liver and peritoneum being the most common site of recurrence. Reith et al.23 reported that 39% of patients with EGIST developed metastatic disease or died from tumors within a short period, suggesting that EGIST was an aggressive type of stromal tumor. In our review, majority (76.5%) of pancreatic EGISTs are classified to the high risk category at the time of diagnosis. Within 30 months after resection, recurrence occurred in 7 (7/17, 41.2%) patients, with hepatic metastasis being more frequent (6/7, 85.7%) than other sites.
Thus, complete surgical resection with negative microscopic margin should be considered as first-line treatment for pancreatic EGIST. Intense surveillance after surgical treatment is advocated. Adjuvant treatment following surgical treatment should be considered to enhance the possibility of curing the cancer. It can prevent recurrences or metastasis because pancreatic EGIST has high potential for malignancy or recurrence.
Our review on pancreatic EGISTs is limited and insufficient to make a conclusion regarding their clinical features. These manifested large masses tended to have aggressive biological and clinical behavior. Therefore, pancreatic EGISTs need to be carefully differentiated from their gastrointestinal counterparts. Adequate surgical intervention and postoperative adjuvant treatment are necessary for EGISTs.


 XML Download
XML Download