

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute cholecystitis is frequently encountered in daily practice, with pain in the right upper quadrant pain being the foremost symptom.12 At times, acute cholecystitis requires emergency treatment for morbidities such as gangrenous cholecystitis, emphysematous cholecystitis, and gallbladder torsion.1234
The first-line treatment for acute cholecystitis is early or urgent cholecystectomy, with laparoscopic cholecystectomy (LC) being the preferred method.1 However, LC is associated with a high incidence of conversion to open cholecystectomy.5 The rate of conversion to open surgery in cases of severe cholecystitis such as gangrenous cholecystitis (one of the more severe forms of acute cholecystitis) is 6% to 35%.6789101112 Besides, some reports have presented several LC complications, including common bile duct (CBD) injury, intra-abdominal abscess, and bile leakage.67
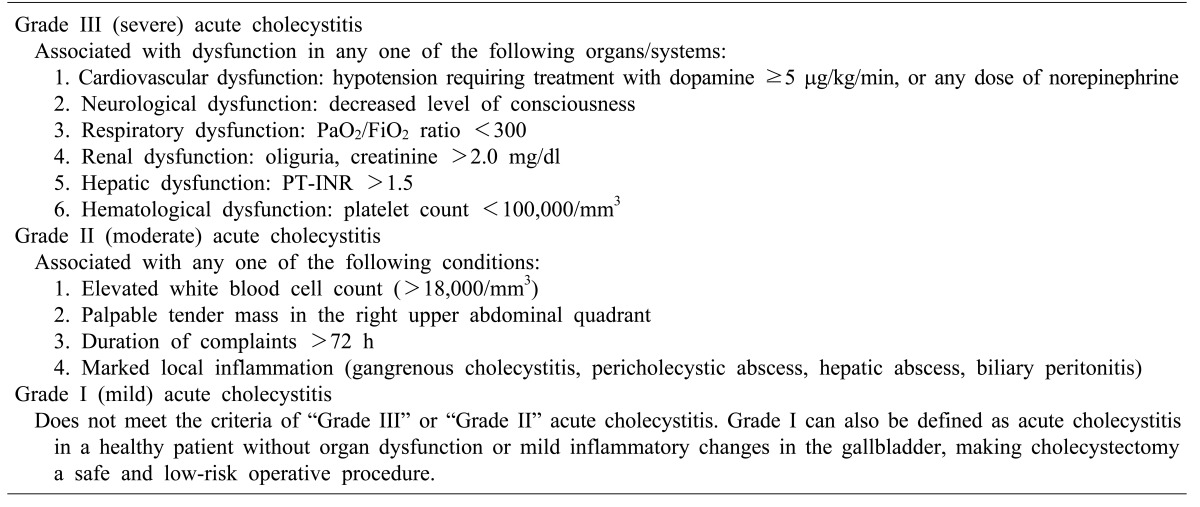
In 1980, percutaneous transhepatic gallbladder drainage (PTGBD) was first applied to patients who developed acute cholecystitis or obstructive biliary disease. Traditionally, it is considered as a safe alternative therapeutic option for resolving acute cholecystitis in surgically high-risk patients with severe comorbidities.11121314 Currently, numerous reports present that PTGBD is a safe and effective procedure that can be used as an immediate treatment in elderly or critically ill patients, before cholecystectomy can be safely performed on improvement of the patient's condition.131415 The Tokyo Guidelines 2007 (TG07) recommended PTGBD is for patients with grade II (moderate) cholecystitis who were unresponsive to conservative treatment, and for patient with grade III (severe) disease.5 Likewise, the updated Tokyo Guidelines 2013 (TG13) recommends PTGBD as a standard drainage method according to the grade system (Table 1).1
In this study, we evaluate the surgical outcomes, effectiveness, and potential advantages of LC for acute cholecystitis by focusing on the differences between early LC without PTGBD, and scheduled LC following PTGBD.
Go to : 
MATERIALS AND METHODS
Study group
We reviewed 1270 patients who underwent LC by a single hepatobiliary surgeon, from March 2010 to December 2014, at the Inje University Haeundae Paik Hospital, Busan, Korea. Of these, 976 patients who underwent LC due to gallbladder stone without cholecystitis, chronic cholecystitis, gallbladder polyp, or gallbladder cancer, were excluded. A total of 294 patients were enrolled in this study and analyzed retrospectively. Among them, 166 patients (56.5%) underwent emergency LC without PTGBD (Group I), and 128 patients (43.5%) underwent scheduled LC following PTGBD.
Diagnosis of acute cholecystitis
Acute cholecystitis was defined according to the TG13 diagnostic criteria: (A) local signs of inflammation (Murphy's sign, right upper quadrant mass/pain/tenderness), (B) systemic signs of inflammation (fever, elevated C-reactive protein, elevated white blood cell count), and (C) imaging findings characteristic of acute cholecystitis (gallbladder distention, pericholecystic fat stranding, gallbladder wall thickening, subserosal edema, pericholecystic fluid collection).12 Computed tomography (CT) scan was performed for all patients with suspicious acute cholecystitis.
Indication and procedure of PTGBD
Indications for PTGBD were grade II (moderate) or grade III (severe) acute cholecystitis according to TG13, or the presence of a significant comorbidity that required further evaluation before surgery.12 PTGBD was selectively performed for patients with grade II or III acute cholecystitis, or with significant comorbidity. PTGBD was performed under local anesthesia, by a single intervention radiologist. Under ultrasound guidance, a 21-gauge Chiba needle was used to puncture the transhepatic gallbladder. Next, using a guidewire under fluoroscopy, an 8.5-Fr pigtail catheter was placed in the gallbladder. Cholangiogram was performed immediately to confirm the correct positioning of the catheter within the gallbladder.
Operative technique
All LCs were performed by a single experienced surgeon using the three-port or four-port method. A 11 mm diameter trocar was inserted into the sub-umbilical area for the laparoscope. Two 5 mm trocars were inserted into the epigastric and right subcostal area for the working devices. As per the requirement, an additional 5 mm trocar was inserted into the right subcostal area. During the operation, the PTGBD catheter was removed after confirming its accurate positioning.
Statistical analysis
Clinical characteristics (such as age, sex, American Society of Anesthesiologists (ASA) classes on admission) and surgical outcomes (including operative time, conversion rate to open surgery, postoperative complications, and duration of hospital stay) were compared between the two groups. Also, the severity of the clinical condition of patients was compared between the groups for each ASA classification.
Statistical analysis was carried out using the SPSS for Windows, version 18.0 (SPSS Inc., Chicago, IL). Differences were considered as statistically significant if p-value was less than 0.05 (p<0.05).
Go to :
RESULTS
Clinical characteristics on admission
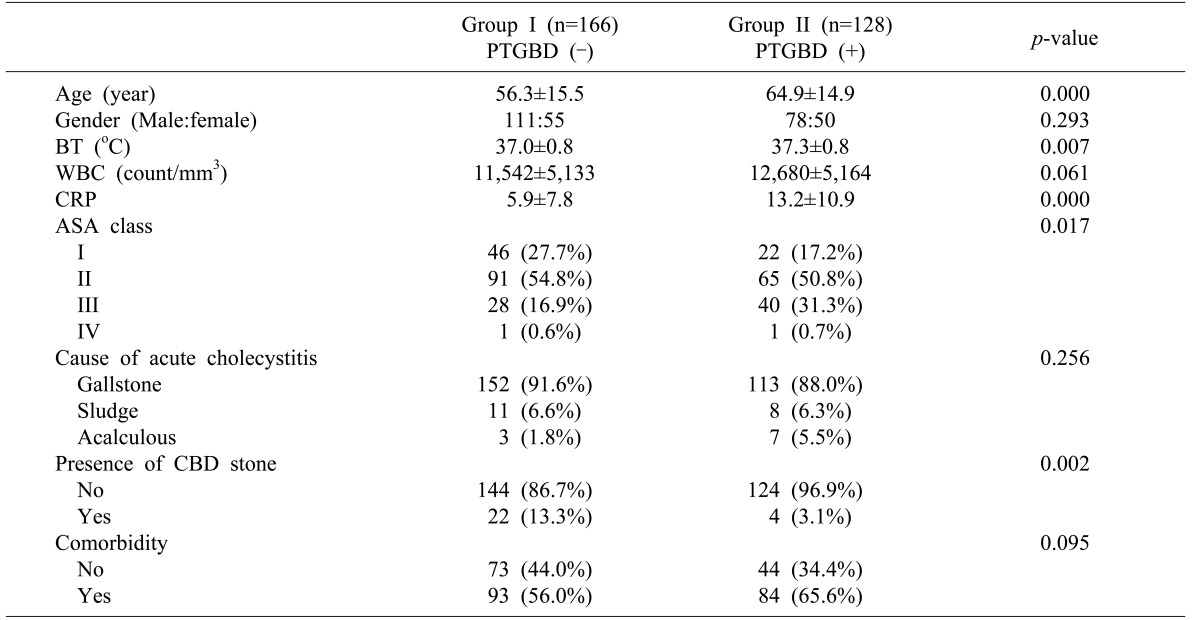
The mean age was 56.3 years in group I and 64.9 years in group II (p<0.05, Table 2). There was no significant difference in gender between the two groups. The mean body temperature was 37.0℃ in group I and 37.3℃ in group II (p<0.05). The mean leukocyte counts were 11,542/mm3 in group I and 12,680/mm3 in group II (p>0.05). The mean level of C-reactive protein (CRP) was 5.9 mg/dl in group I and 13.2 mg/dl in group II (p<0.05). Based on ASA class, there were a greater (p<0.05) number of high-risk patients in group II than in group I. Gallstone was the main cause of acute cholecystitis in both groups: 152 cases (91.6%) in group I and 113 cases (88.0%) in group II (p>0.05). Additionally, common bile duct stone was present in 22 cases (13.3%) in group I and 4 cases (3.1%) in group II (p<0.02). The rate of patients with comorbidity in Group II (65.6%) was higher than that Group I (56.0%). However, the difference was not statistically significant (p>0.05). PTGBD-related complications were observed in 4 (3.1%) cases; these included pneumothorax, omental hematoma and malposition.
Perioperative surgical outcomes
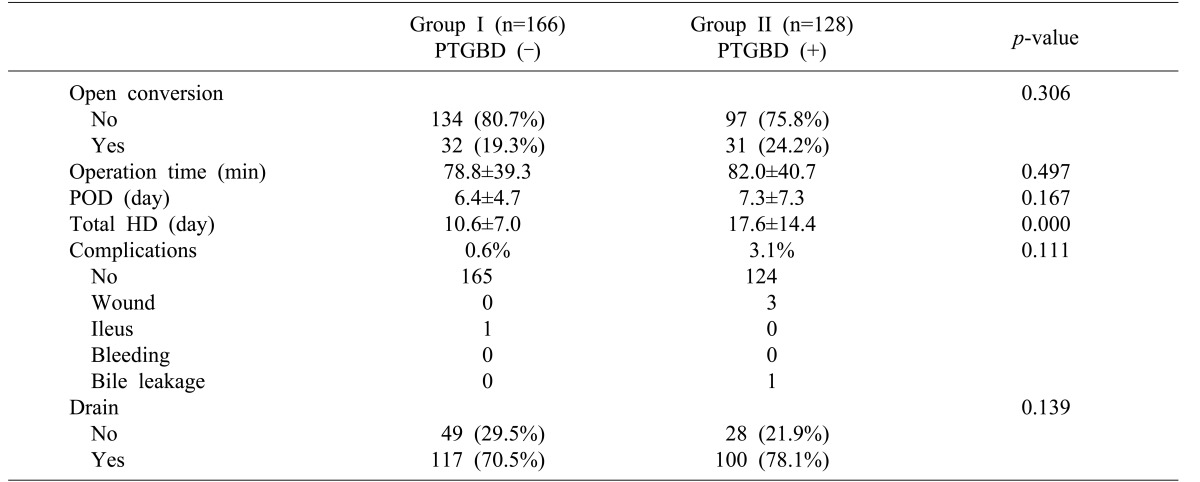
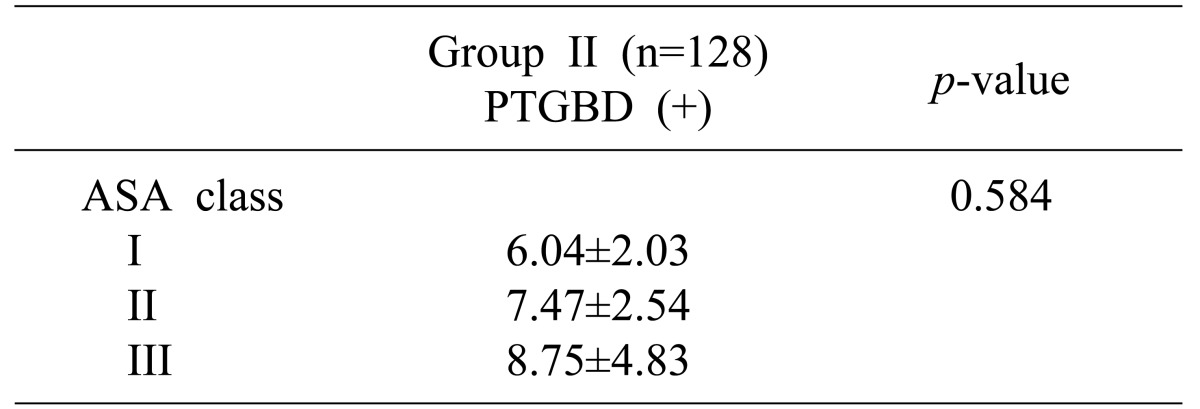
The overall perioperative surgical outcomes in the two groups are summarized in Table 3. Briefly, the perioperative surgical outcomes for group I and group II, respectively, are as follows: conversion rate to open surgery was 19.3% (n=32) and 23.4% (n=30) (p<0.05); mean operative time was 78.8 minutes and 82.0 minutes; period of postoperative hospital stay was 6.4 days and 7.3 days (p<0.05); and postoperative complication rate was 0.6% (n=1) and 3.1% (n=4) (p>0.05). The differences in the overall outcomes were statistically not significant, except total length of hospital stay. The mean total length of hospital stay was 10.6 days in group I and 17.6 days in group II (p<0.05). One patient in group I had complications involving the ileus. In Group II, complications with wound problem or bile leakage were reported in 4 cases. All complications developed after conversion from LC to open surgery. The patients in group II underwent scheduled cholecystectomy 7.61±3.46 (2-23) days after PTGBD insertion, and no difference was noted between each ASA classes (p>0.05, Table 4).
Comparison between the two groups according to the American Society of Anesthesiologists classes
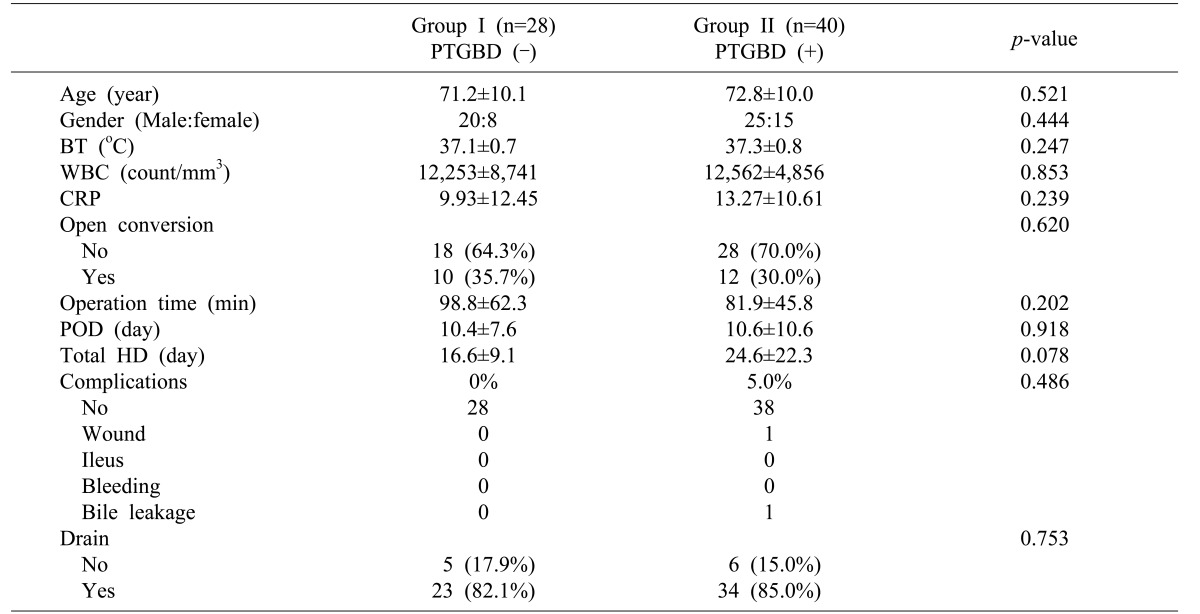
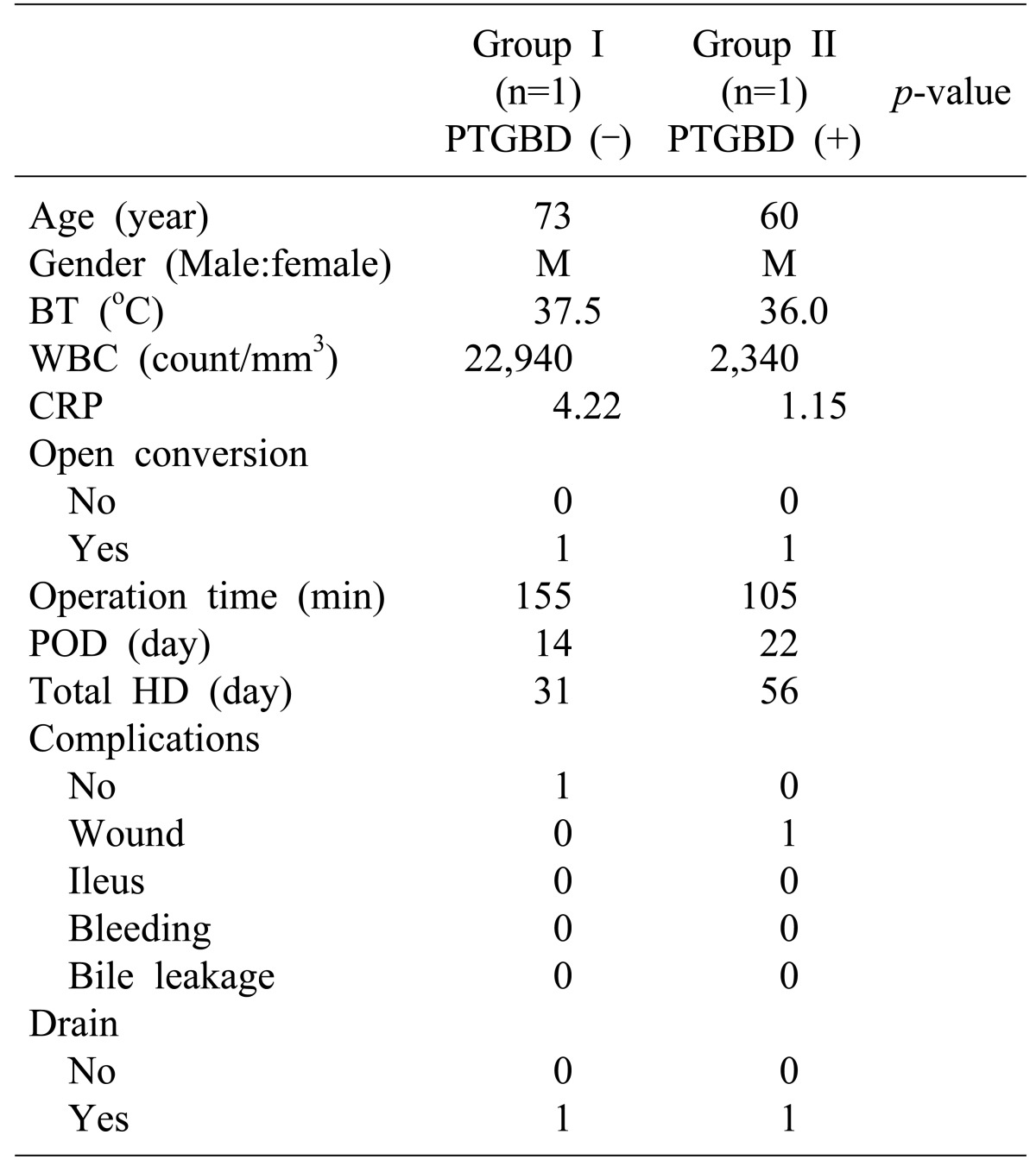
Group I and group II were further analyzed according to each ASA class (Tables 5,6,7,8). For patients with ASA class 1, the mean body temperatures, mean CRP levels, and total length of hospital stay in group II were significantly greater (p<0.05) than those in group I. However, there was no significant difference in other clinical characteristics or surgical outcomes between the two groups (Table 5). For patients with ASA class 2, the mean age, mean leukocyte counts, mean CRP levels, and total lengths of hospital stay in group II were significantly greater (p<0.05) than those in group I. All other clinical characteristics and surgical outcomes of the two groups were similar (Table 6). For patients with ASA class 3, no remarkable difference was observed in the conversion rate to open surgery, operative time, postoperative complication rate, or postoperative hospital stay between the two groups (Table 7). One patient in each group was classified as ASA class 4. Both patients underwent open conversion (Table 8).
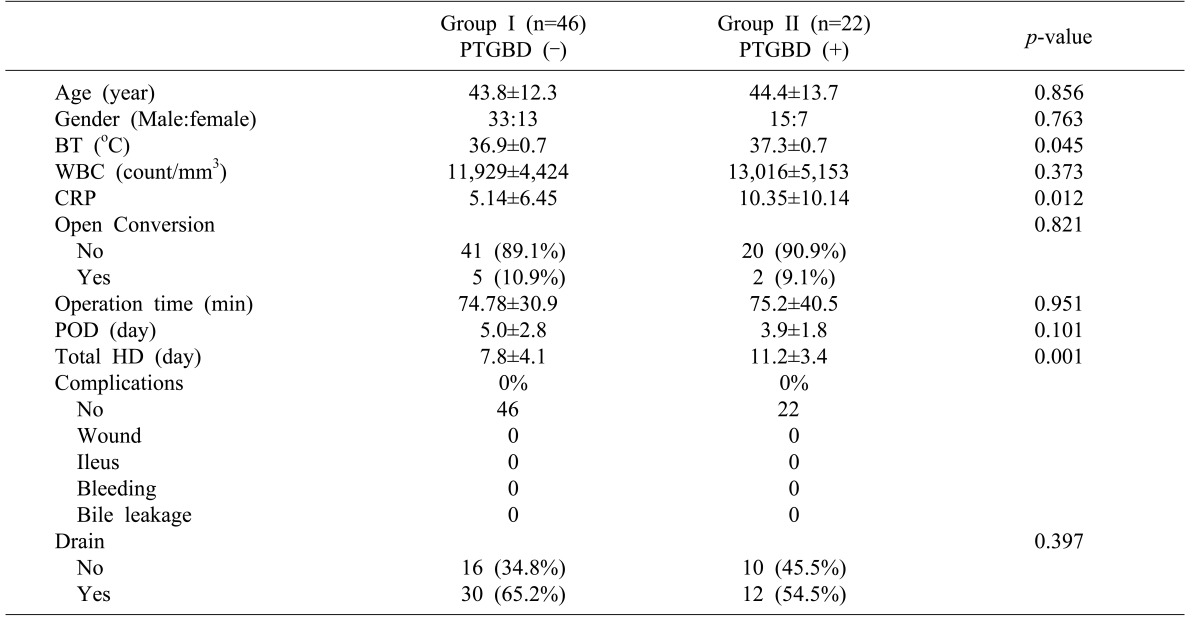
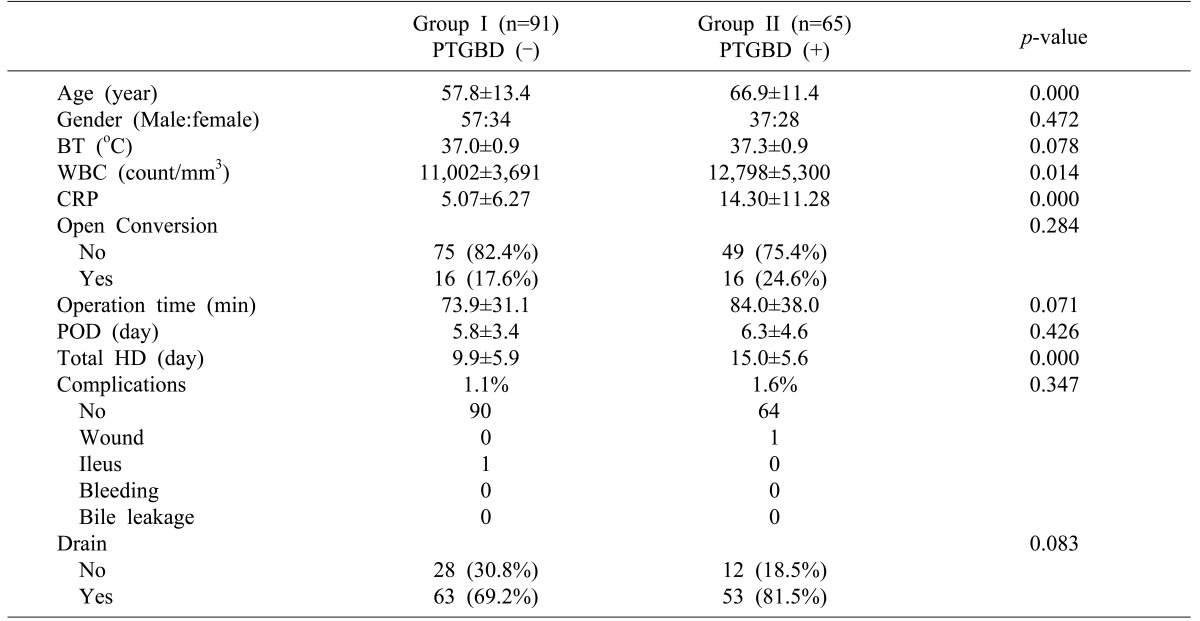
Table 5
Comparison between the two groups as per the American Society of Anesthesiologists Class I (ASA I)
![]()
Table 6
Comparison between the two groups as per the American Society of Anesthesiologists Class 2 (ASA II)
![]()
Go to :
DISCUSSION
In TG07, PTGBD was recommended only for patients with grade II (moderate) cholecystitis unresponsive to conservative treatment, and for patients with grade III (severe) disease.8 Recently, several alternate methods for biliary drainage have been introduced, such as percutaneous transhepatic gallbladder aspiration (PTGBA), endoscopic naso-biliary gallbladder drainage (ENGBD) and endoscopic gallbladder stenting (EGBS).910 However, these alternatives have not been fully evaluated for their effectiveness in patients with acute cholecystitis. According to TG13, PTGBD is still recognized as the standard drainage method for surgically unfit patients with acute cholecystitis.11
Before the 2007 publication of the Tokyo Guidelines for the management of acute cholangitis and cholecystitis (TG07), there were no diagnostic or severity assessment criteria for acute cholecystitis.8 The Tokyo Guidelines Revision Committee for the revision of TG07 (TGRC) developed new diagnostic criteria and severity assessment criteria by retrospectively analyzing cases of acute cholecystitis. Hence, the final draft of the updated Tokyo Guidelines (TG13) was prepared based on evidence from retrospective multi-center analysis. The TG13 improved the diagnostic sensitivity for acute cholecystitis, and presented criteria with extremely low false positive rates adapted for clinical practice.9
The optimal timing for cholecystectomy in patients with acute cholecystitis has been controversial in the past decades. Even though LC plays a major role in the treatment of acute cholecystitis, there is an ongoing debate regarding the optimal timing for the surgery.161718 PG13 has recommended management of acute cholecystitis based on its severity. Early LC is the first-line treatment for patients with Grade I (mild) acute cholecystitis. For patients with Grade II (moderate) acute cholecystitis, delayed/elective laparoscopic cholecystectomy after initial medical treatment with antimicrobial agent is the recommended first-line treatment. In non-responders to the initial medical treatment, gallbladder drainage should be considered. For patients with Grade III (severe) acute cholecystitis, appropriate organ support, in addition to initial medical treatment, is necessary. In such situations, urgent or early gallbladder drainage is recommended.1 Elective cholecystectomy can be performed after treating the acute inflammatory process.13 Although an operation within the golden 72 hours from symptom onset has been suggested, early surgery is not always possible in clinical practice due to logistic difficulties in performing an emergency surgery for such patients.10192021 Furthermore, emergency surgical procedures could lead to serious complications in high-risk patients.10
Many reports state that it is easier to perform surgery for acute cholecystitis within 24 to 72 hours after the first onset of symptoms.18192021 In cases of PTGBD following scheduled LC, Choi et al.22 reported a group of patients who underwent delayed LC at 5 days after PTGBD, had better results than the group who underwent LC within 72 hours after PTGBD. Han et al.23 also reported that the perioperative complication rate in a group of patients who underwent LC within 72 hours after PTGBD was higher than the group who underwent LC at more than 72 hours after PTGBD. In our hospital, the LCs in group I (without PTGBD) were performed at a mean time of 4.0 days after admission, while LCs in group II (with PTGBD) were performed at a mean time of 9.6 days after admission (8.2 days after PTGBD insertion). The interval from PTGBD insertion to scheduled cholecystectomy in group II was about 7 days.
The usefulness of PTGBD for patients with acute cholecystitis has been endorsed in many case-series studies, but there are not in proper controlled trials.111213141516 Mortality rates after cholecystectomy in elderly patients with acute cholecystitis are reportedly lower than those recorded in previous years.24 Recent advances in anesthesiology and perioperative care have improved the outcomes of cholecystectomy for critically ill patients. However, there have been no randomized controlled studies to evaluate the outcomes of PTGBD versus early cholecystectomy.12
In general, LC in patients with acute cholecystitis is difficult, due to the possibility of an adjacent organ injury. Acute inflammation in patients with acute cholecystitis begins with distention of the gallbladder and edematous change in the gallbladder wall. Subsequently, acute cholecystitis gradually progresses to empyema, perforation, and abscess formation.25 Lo et al.26 showed that there is no difference in terms of operative time, blood loss, conversion, or complication rate among early open cholecystectomy group, early LC group, and elective LC after PTGBD group. On the other hand, Chikamori et al.27 reported that the early scheduled LC following PTGBD group has a lower conversion rate to open cholecystectomy with shorter operative time, as compared to the early LC without PTGBD group, or delayed LC after conservative therapy group. Kim et al.28 have also reported that elective delayed LC after PTGBD group has a lower conversion rate and complication rate. In this study, no statistical difference was observed between the two groups in the aspect of postoperative complications. All complications in Group II occurred after open conversion. Especially to be noted was a case of bile leakage after partial cholecystectomy. Occasional bile leakage from PTGBD inserted site is known to occur. Removal of the PTGBD after laparoscopic inspection and examination of the site for bile leakage, could help in preventing this complication. If bile leakage is detected, the leakage site should be immediately closed by intracorporeal suturing. For these reasons, we consider PTGBD in patients with acute cholecystitis as a useful procedure for laparoscopic surgery, since it decompresses the gallbladder distention and attenuates the wall and pericholecystic inflammation, in spite of longer preoperative hospital stay in clinical practice.
Based on this study, grade II (moderate) or grade III (severe) acute cholecystitis (according to TG13), as well as the presence of a significant comorbidity that required further evaluation before surgery, were suitable candidates for PTGBD insertion. Consequently, such selection bias might have affected the outcomes in this study. To exclude selection bias, we compared the outcomes of two groups according to ASA classes, but obtained similar results. However, some reports show that PTGBD following LC has a significantly better outcome, such as the conversion rate to open surgery, postoperative complications and other perioperative surgical outcomes for patients with severe comorbidities.2930
In some instances, surgery was delayed because the operating room or hepatobiliary surgery specialist was not available. At other times, the intervention specialist was not available. Moreover, some patients with acute cholecystitis were admitted to the Department of Gastroenterology for conservative treatment or other procedures, such as endoscopic retrograde cholangiopancreatography (ERCP). Due to these reasons, surgery was delayed in many cases. Such situations might have also affected the outcomes of surgery.
In cases with severe cholecystitis, the rate of conversion to open surgery has been reported ranging from 8.7% to 35%.7212830 Merriam et al.31 reported that early LC for acute gangrenous cholecystitis has a relatively high conversion rate (35%) than nongangrenous cholecystitis (6%). Our data showed that the conversion rate was 19.3% in Group I and 24.2% in Group II (p>0.05). This difference in results could be due to a single surgeon, who tried to avoid bias in diversity regarding the criteria for conversion to open surgery. Therefore, consensus about the criteria for open conversion is needed by undertaking a large multicenter study in the future.
In conclusion, scheduled LC following PTGBD insertion did not reduce the rate of open conversion or postoperative hospital stay, compared to emergency LC without PTGBD. Outcomes were also similar according to ASA classes for comorbidity, when compared with emergency LC without PTGBD. Since this study is retrospective in nature, it might have bias in the selection of patients who had undergone PTGBD. Further large multi-center randomized study is required to avoid selection bias, and to confirm the indication for PTGBD or early cholecystectomy. However, in clinical practice, scheduled LC following PTGBD is important for patients having acute cholecystitis with concurrent comorbidity.
Go to :
 XML Download
XML Download