

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Small cell carcinoma (SCC) is an extremely rare tumor in the gallbladder (GB), that was first described by Albores-Saavedra et al.1 To the researchers' knowledge, less than 100 cases have been published in English literature. Patients with this condition present with aggressive features and early metastasis. Due to the late stage presentation and highly malignant potential, the survival rate for SCC of the GB is low. The median survival time has been reported at nine months.2 The treatment strategy is not clear, but patients with limited disease of the GB can be managed with multimodal therapy, which includes resection and chemoradiation.3 Herein, this study presents a case of SCC of the GB in a patient, who survived for more than 75 months after resection and chemotherapy.
CASE
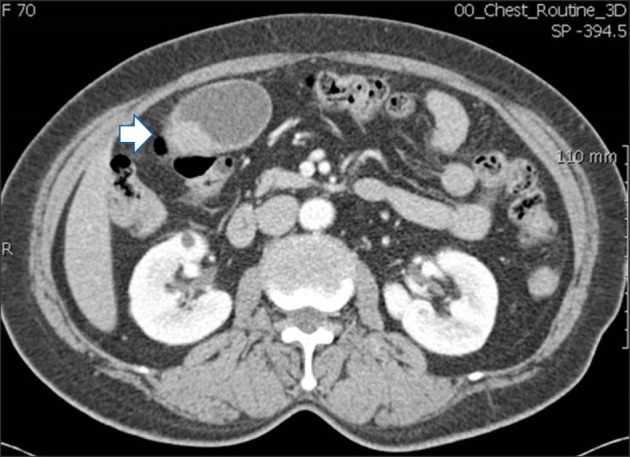
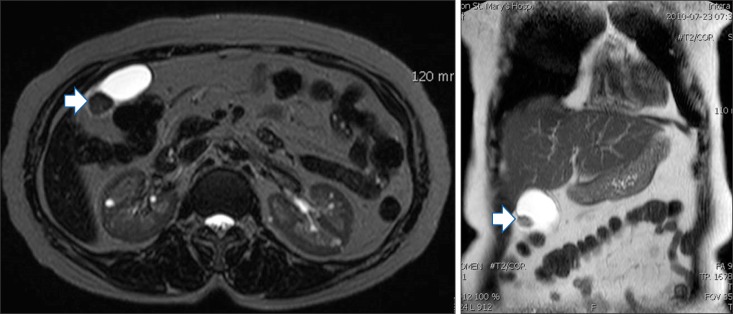
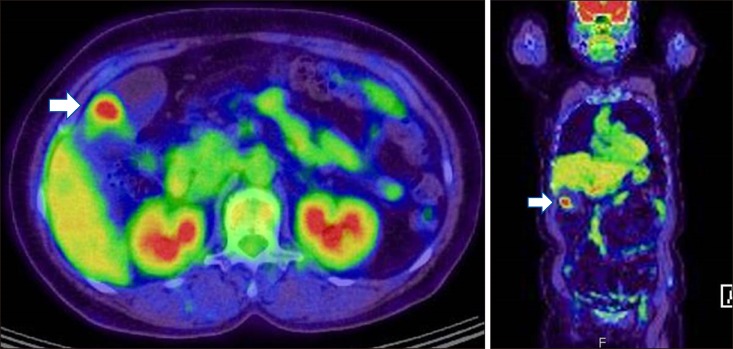
A 70-year-old had a gallstone which was identified two years prior. She had a mass in the GB, which was not accompanied by any symptoms. One month before admission, the patient was examined with computed tomography (CT) (Fig. 1), due to pneumonia, and a mass in the GB was detected incidentally. After recovering from pneumonia, magnetic resonance cholangiopancreatography (MRCP), and positron emission tomography (PET)-CT were performed. A 2.6 cm mass in the GB, with an enlarged lymph node at the hepatic hilum, was found without any distant metastasis (Figs. 2 and 3). The blood chemistry results were within the normal limits and tumor markers (carcinoembryonic antigen and Cancer Antigen 19-9) were not elevated.
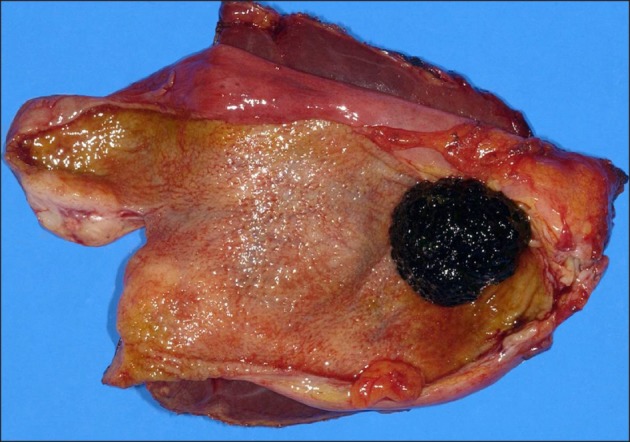
A radical cholecystectomy which included liver wedge resection, cholecystectomy, and regional lymph node dissection was performed. During the operation, the gross findings showed a 3×3 cm-sized mass on the fundus of the GB, on the opposite side of the liver fossa. The mass did not perforate the serosa and a black-pigmented stone was identified in the GB (Fig. 4). The frozen sections of a cystic lymph node and the tissue of the mass were malignant. Subsequent frozen sections of the resected margin of the cystic duct and lymph nodes along the common bile duct and the hepatic artery were negative.
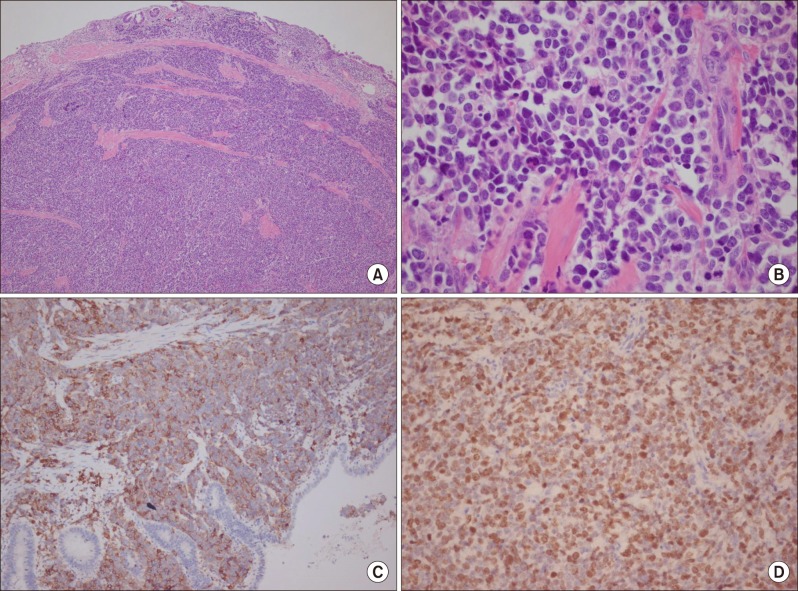
The tumor showed a finding consistent with poorly differentiated SCC of the GB. Tumor cells were positive for chromogranin A, synaptophysin, and Ki-67 (Fig. 5). Metastases were present in two lymph nodes, leading to a score of T2N1M0 and stage IIIB (AJCC 7th). The patient received six cycles of chemotherapy, which consisted of etoposide and cisplatin. Seventy-five months after the operation, the patient is well, without recurrence.
DISCUSSION
Neuroendocrine tumors (NETs) are a rare, heterogeneous group of tumors. These tumors predominantly occur in the bronchopulmonary system, pancreas, and gastrointestinal system. NETs secrete humoral agents that cause distinct clinical syndromes, including carcinoid syndrome. Most NETs are clinically silent, until late presentation with mass effects.4 Although various proposals for the classification and nomenclature of NET have been made, they have not been standardized. Most systems categorize NET by location, differentiation, and grade (proliferative rate) of the tumor.5 Small- and large-cell carcinomas are high-grade and poorly differentiated.
The incidence of SCC of the GB is approximately 0.5% of all GB cancers, where the most common carcinoma is adenocarcinoma.6 Among NETs of the gastrointestinal tract, SCC of the GB compromises 0.2%.7 Less than 100 cases of this tumor have been published in the English literature, since Albores-Saavedra et al.1 described it first in 1981. It usually occurs in elderly women and often accompanies cholelithiasis. Moreover, this condition presents at a late stage at diagnosis. About two-thirds of patients are diagnosed at stage IV. The median survival period is nine months. The common sites of metastases are the lymph nodes, liver, and lungs.28 There have been no reports about SCC of the GB with carcinoid syndrome or other symptoms caused by biologically active peptides.
Reports about the management of SCC of the GB are scarce. Not only is it an extremely rare tumor, but the late stages at presentation due to its aggressiveness, also make it difficult to establish protocols for its management. Surgery is the mainstay of GB cancer treatment, but it is unclear whether radical operations produce better outcomes for advanced stages of SCC. Groeschl et al.3 analyzed the SEER (The Surveillance, Epidemiology, and End-Results) database between 1998 and 2008, in a study of hepatopancreatobiliary SCC, and concluded that surgical resection was associated with prolonged survival for patients with localized pancreatobiliary SCC. Of 32 patients with SCC of the GB, 24 (75%) received surgery. Prolonged overall survival was observed in the group undergoing an operation (18 months vs. 9 months).
Due to poor prognosis of SCC of the GB, regardless of the possibility of curative surgery, additional modalities including chemoradiation should be considered. As with pulmonary SCCs, etoposide plus cisplatin has had some effectiveness in patients with SCC of the GB. As reported previously,249 gemcitabine can be administered with platinum agents.10 Streptozocin with fluorouracil or doxorubicin was reported to benefit pancreatic NETs. Some new drugs that target angiogenesis and intracellular signal pathways are under currently assessment for gastroenteropancreatic NETs.4 Although there is little experience with radiation for patients with SCC of the GB, it can be considered for use postoperatively, or to ameliorate symptoms, which are caused by an unresected tumor or metastasis.3
SCC of the GB has an extremely low incidence and poor prognosis. Early diagnosis and aggressive treatment including resection and chemoradiation have been reported to produce the best clinical outcomes. In this case, the researchers performed radical cholecystectomy and administered adjuvant chemotherapy in a patient with SCC of the GB. She has survived for 75 months after the operation. The researchers hope that further advances in multimodal therapy will improve the survival rates of SCC of the GB.
 XML Download
XML Download