

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The purpose of this study was to compare desflurane anesthesia with desflurane-remifentanil anesthesia by measuring postoperative pain, nausea and vomiting after gynecologic laparoscopic surgery.
Methods
Data were collected using a random double blind method. The experimental group treated with desflurane-remifentanil anesthesia had a total of 25 patients. The control group had 20 patients who were treated with desflurane anesthesia. Pain (VAS), pushing PCA button, nausea and vomiting (VAS) were assessed at PACU (Post Anesthesia Care Unit) arrival, 10 min, 20 min, 30 min in PACU and 2 hrs, 6 hrs, 24 hrs, 48 hrs in ward. INVR was assessed at 24 hrs. Extra analgesics and extra antiemetics were measured in PACU and the ward. Data were analyzed using t-test and repeated measure using ANOVA.
Results
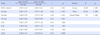
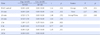
The experimental group presented with more postoperative pain (F=7.55, p<.001) than the control group. The experimental group took more extra analgesics in PACU and pressed the PCA button more often for 6 hours. The experimental group complained more postoperative nausea (F=2.11, p=.043) than the control group and took extra antiemetics during postoperative period of 24 hours.
Figures and Tables
Table 1
Research Design

Exp.=experimental group, Cont.=control group; E1,C1=Pretests of get research permission, History taking of nausea (VAS), Assess pain (VAS); PACU a=Post Anesthesia Care Unit arrival; E2,E3,E4,C2,C3,C4=Posttests of assess pain (VAS), Nausea (VAS); E5,E6,E7,E8,E9,C5,C6,C7,C8,C9=Posttests of assess pain (VAS), Nausea (VAS), Frequency of pushing; PCA (Patient Controlled Anesthesia) button; E5,C5=Total Counts of additional drugs (analgesics and antiemetics) in PACU; E8,C8=assess Index of Nausea, Vomiting & Retching (INVR); E9,C9=Total Counts of additional drugs (analgesics and antiemetics) in Ward.
![]()
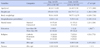
Table 2
Homogeneity Test for General Characteristics, Preoperative Pain and Nausea between Experimental and Control Group (N=45)
![]()
Table 3
Comparison of Postoperative Pain between Experimental and Control Group (N=45)
![]()
Table 4
Comparison of Frequency of Pushing PCA Button and Administration of Extra Analgesics between Experimental and Control Group (N=45)

![]()
Table 5
Comparison of Nausea between Experimental and Control Group (N=45)
![]()
Table 6
Comparison of INVR and Administration of Extra Antiemetics between Experimental and Control Group (N=45)

![]()
Summary Statement
▪ What is already known about this topic?
Remifentanil combined with inhalation anesthetics such as sevoflurane might cause pain and nausea after surgery however, this is still being debated. Studies conducted using desflurane-remifentanil combination anesthetics were not found in the literature review.
▪ What this paper adds?
The experimental group presented with more postoperative pain than the control group. The experimental group took more extra analgesics in PACU and pressed the PCA button more often for 6 hours. The experimental group complained more postoperative nausea than the control group and took extra antiemetics during postoperative period of 24 hours.
▪ Implications for practice, education and/or policy
Desflurane-remifentanil anesthesia requires more careful nursing intervention in post-operative pain management until 6 hours and post operative nausea management until 24 hours.
References
1. Choi JY, Song JI, Whang BC, Lee SP, Choi YD, Park CY, et al. A clinical study on 570 cases of laparoscopy assisted vaginal hysterectomy (LAVH). Korean J Obstet Gynecol. 2004; 47(10):1954–1959.
2. Kang HS, Park HJ. Comparison of postoperative pain after abdominal and laparoscopic assisted vaginal hysterectomy by using IV-PCA. Korean J Anesthesiol. 2007; 52(3):301–305.

3. Son MK, Lee GY, Kim CH, Chung RK. The effects of midazolam and remifentanil on induction of anesthesia and hemodynamics during tracheal intubation under target-controlled infusion of propofol. Korean J Anesthesiol. 2009; 56(6):619–623.
4. Kim SK, Kim DK, Son JS, Ko SH, Lee JR. What is the optimal effect-site concentration of remifentanil for minimizing the cardiovascular changes to endotracheal intubation during induction with propofol? Korean J Anesthesiol. 2008; 54(1):30–36.
5. Lee JH, Kim SI, Kim MG, Kim SC, Ok SY. The influence of remifentanil on the bispectral index during intubation under TIVA using propofol. Korean J Anesthesiol. 2007; 53(6):695–699.
6. Kim TH, Choi IC, Kang SJ, Kim JS, Jeong YB. Intravenous Patient-controlled Analgesia using Remifentanil after Cardiac Surgery. Korean J Anesthesiol. 2007; 53(6):740–745.
7. Lee EM, Lee H, Kim CH, Lee GY. A double-blinded, randomized, placebo controlled study of the effect a small dose of ketamine has on postoperative pain of sevoflurane-remifentanil anesthesia. Korean J Anesthesiol. 2008; 54(2):146–151.
8. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: Results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003; 97(2):534–540.
9. Dolin SJ, Cashman JN, Bland JM. Effectiveness of acute postoperative pain management: I. Evidence from published data. Br J Anaesth. 2002; 89(3):409–423.
10. Guignard B, Bossard AE, Coste C, Sessler DI, Lebralt C, Alfonsi P, et al. Acute opioid tolerence: Intraoperative remifentanil increases postoperative pain and morphine requirement. Anesthesiology. 2000; 93(2):409–417.
11. Vinik HR, Kissin I. Rapid development of tolerance to analgesia during remifentanil infusion in humans. Anesth Analg. 1998; 86(6):1307–1311.
12. Crawford MW, Hickey C, Zaarour C, Howard A, Naser B. Development of acute opioid tolerance during infusion of remifentanil for pediatric scoliosis surgery. Anesth Analg. 2006; 102(6):1662–1667.
13. Gustorff B, Nahlik G, Hoerauf KH, Kress HG. The absence of acute tolerance duringremifentanil infusion in volunteers. Anesth Analg. 2002; 94(5):1223–1228.
14. Cortinez LI, Brandes V, Munoz HR, Guerrero ME, Mur M. No clinical evidence of acute opioid tolerance after remifentanilbased anesthesia. Br J Anaesth. 2001; 87(6):866–869.
15. Cho AR, Kim HK, Kim KH, Jung KY, Kim WS, Kwon JY. Effect of remifentanil on postoperative pain in gynecologic surgery with sevoflurane anesthesia. Korean J Anesthesiol. 2008; 55(2):182–189.
16. Myles PS, Williams DL, Hendrata M, Anderson H, Weeks AM. Patient satisfaction after anesthesia and surgery: Results of a prospective survey of 10,811 patients. Br J Anaesth. 2000; 84(1):6–10.
17. Kang DH, Lee JG, Jung HJ, Kim JD, Yu SB, Ryu SJ, et al. A comparison of the recovery characteristics between propofol-remifentil and Sevoflurane-remifentail anesthesia for total thyroidectomy. Kosin Med J. 2013; 28(2):137–143.
18. Kim GH, Ahn HJ, Kim HS, Bang SR, Cho HS, Yang M, et al. Postoperative nausea and vomiting after endoscopic thyroidectomy: Total intravenous vs. balanced anesthesia. Korean J Anesthesiol. 2011; 60(6):416–421.
19. Wikipedia. Visual Analogue Scale [Internet]. cited 2010 January 1. Available from http://en.wikipedia.org/wiki/Visual_analogue_scale.
20. Rhodes VA, McDaniel RW. The index of nausea, vomiting, and retching: A new format of the index of nausea and vomiting. Oncol Nurs Forum. 1999; 26(5):889–894.
21. Kim YJ, Kim JY, Choi IR, Kim MW, Rhodes V. The index of nausea, vomiting, and retching(Korean translation). J Korean Acad Adult Nurs. 2000; 12(2):278–285.
22. Kim YS, Lee WK, Choi YS, Chae YK, Ahn SW, Lee A, et al. A comparison of the recovery characteristics of propofol-remifentanil and desflurane-remifentanil anesthesia under bispectral index (BIS) monitoring following laparoscopic cholecystectomy. Anesthesia and Pain Medicine. 2011; 6(4):331–335.
23. Roberts GW, Bekker TB, Carlsen HH, Moffatt CH, Slattery PJ, McClure AF. Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth Analg. 2005; 101(5):1343–1348.
24. Watcha MF, White PF. Postoperative nausea and vomiting. It's etiology, treatment, and prevention. Anesthesiology. 1992; 77(1):162–184.
25. Glass PS, Gan TJ, Howell S. A review of the pharmacokinetics and pharmacodynamics of remifentanil. Anesth Analg. 1999; 89:4 Suppl. S7–S14.
26. Dershwitz M, Michalowski P, Chang Y, Rosow CE, Conlay LA. Postoperative nausea and vomiting after total intravenous anesthesia with propofol and remifentanil or alfentanil: How important is the opioid? J Clin Anesth. 2002; 14(4):275–278.
 XML Download
XML Download