

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Aneurysmal subarachnoid hemorrhage is rare in the pediatric population.5) Cerebral vasospasm (CV) can be seen in 50-80% of these patients, however, delayed ischemia is rarely seen due to robust collateral circulation.3)4) In patients with severe or symptomatic CV despite medical management, intra-arterial vasospasm therapy or balloon angioplasty can be performed safely.3) We present an infant with CV, treated with a modified Dotter technique to perform mechanical angioplasty of the intracranial arteries refractory to intra-arterial verapamil and in whom balloon angioplasty could not be safely performed.2)
CASE REPORT
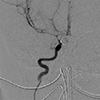
An 8-month old female presented with acute subarachnoid hemorrhage due to a four-millimeter paraclinoid ruptured aneurysm of the right internal carotid artery (ICA). She was treated successfully with endovascular coiling of the aneurysm. Trans-cranial Doppler ultrasound (TCD) performed in four days following the rupture demonstrated mean middle cerebral artery (MCA) velocities greater than 330 cm/sec on the right and greater than 160 cm/sec on the left. The patient showed no focal neurological deficit, though she was sedated using fentanyl in the intensive care unit during this time. On the following day, mean velocities of all intracranial vessels on TCD increased despite medical management, with mean velocities greater than 350 cm/sec in all intracranial arteries on the right and greater than 200 cm/sec in arteries on the left. The patient was taken to the angiography suite for cerebral angiogram and possible angioplasty. Vascular access was obtained, and the patient was heparinized with a dose of 60 units/kg. The angiogram revealed vasospasm of the supraclinoid ICA, MCA, and anterior cerebral artery (ACA) territories bilaterally of greater than 60% in diameter if all intracranial arteries when compared to her initial angiogram (Fig. 1). The proximal segments of right and left MCA segments, in particular, were 0.6 and 0.5 mm in diameter, respectively (compared to roughly 1.5 mm on original angiogram in both MCAs). Intra-arterial verapamil was administered, however, after 15 minutes, follow-up angiogram revealed persistent vasospasm. Balloon angioplasty was then attempted using a 1.5 mm “over-the-wire” balloon through a 5F guide catheter, but the device could not be advanced safely through the ICA due to the small size of the patient's intracranial vessels.
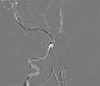
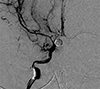
Therefore, a microcatheter (Marathon™ Microcatheter [Covidien, Irvine, CA, USA]; 0.0165" diameter) was advanced over a J-shaped 0.014" soft microwire (Mirage™ Microwire, Covidien, Irvine, CA, USA) under roadmap guidance to mechanically dilate the supraclinoid ICA and MCA bilaterally (Fig. 2). The microwire was formed into a tight J-shape in order to decrease the risk of vessel perforation and was tracked into the MCA without need for excessive forward tension. The microcatheter was then brought into the MCA vessels over the wire without incident. By passing the microwire and subsequently the microcatheter, sequential mechanical angioplasty of the vessel was performed. Dramatic improvement was seen angiographically in that the proximal MCA M1 segment diameters increased to 1.0 and 1.2 mm, right and left (Fig. 3). Mean TCD velocities decreased to below 200 cm/sec in all vessels the following day, and continued to trend down thereafter. Follow-up angiography demonstrated a 66% and 140% improvement in the degree of stenosis in the right and left MCA, respectively (2/3 of their initial diameter). However, angioplasty of the ACA A1 segments, though also in severe angiographic vasospasm, was not attempted due to the increased risk of vessel perforation during catheterization. ACA TCD mean velocities decreased following the procedure.
There were no complications from the procedure and follow-up magnetic resonance imaging the following day demonstrated no ischemic injury and no apparent vasospasm.
DISCUSSION
Dotter and Judkins successfully performed a catheter angioplasty of an occluded popliteal artery in an elderly patient, achieving revascularization via a sequential system of coaxial catheters.2) Although this procedure may seem elementary when compared to modern neurointerventional techniques and devices, it remains an effective tool in the neurointerventionalist's armamentarium when other treatments fail. This is especially true in the pediatric population, where small vessel diameters often preclude the use of most guide catheters and many transluminal devices. Our patient did not appear to have symptomatic vasospasm, but demonstrated severe CV in all anterior circulation vessels using commonly accepted criteria for adults (mean velocities > 120 cm/sec).1) The pre-vasospasm MCA M1 diameter was at the lower size limit of currently available percutaneous transluminal angioplasty balloons, and as we anticipated, they could not be delivered safely to the vessels of interest. Therefore, we believed that employing a similar technique, as the one performed by Dotter and Judkins2) was inevitable in our patient, despite the high risk of dissection or vasospasm aggravations.
In our practice with adult patients and older children, verapamil and nitroglycerine are our agents of choice due to drug response and our experience in dosing these drugs. Because the patient in this case was so small, we elected to proceed with mechanical angioplasty given the lack of response to verapamil and concerns regarding systemic effects on such a small child with increased use of calcium channel blockers or other agents. Initially, we attempted intra-arterial verapamil to chemically treat our patient's vasospasm; however, after 15 minutes, follow-up angiogram showed that the vasospasm persisted. By this time, vasodilation due to calcium channel blocker effect should have been observed based on considerable prior experience in adult patients. Although we cannot state with certainty that a delayed response to verapamil had no role in the observed improvement in vasospasm, we believe this to be highly likely based on our experience with adults and older children.
As previously mentioned, by passing the microwire and subsequently the microcatheter, sequential mechanical angioplasty of the vessel was performed. This technique was highly successful, and the patient's vasospasm resolved on follow-up angiogram, mean TCD velocities in all anterior circulation arteries improved immediately, and follow-up imaging revealed no ischemia. While the MCA was dilated using the modified Dotter technique, there is a possibility that the associated ACA velocities would have stayed elevated. Had this occurred, we would have revisited the risks and benefits of administering additional vasodilators or attempting mechanical angioplasty of the ACA. However, we believe that navigating the microwire and microcatheter into the MCA from the ICA is substantially less risky as compared to ACA catheterization for two reasons: (1) the natural curvature of the ICA terminus is directed toward the larger caliber MCA which allows, and (2) maintenance of a “J” curvature on the distal wire while advancing it into the MCA. To access the ACA, the wire tip must be used to direct the wire into the A1 segment from the ICA, which can lead to vessel perforation.
CONCLUSION
Overall, this case report highlights a novel modification of an existing technique to safely treat CV in an infant due to aneurysmal subarachnoid hemorrhage becauae balloon angioplasty was not available and chemical angioplasty was ineffective. The use of mechanical angioplasty-a modified Dotter technique-with modern microcatheters and microwires can provide excellent angiographic and clinical outcomes in this setting.
 XML Download
XML Download