

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Alongside with the posterior communicating cerebral artery and middle cerebral artery of bifurcation, the anterior communicating cerebral artery (A com) is one of the most frequent sites of intracranial aneurysm rupture. In the majority of previous studies, however, only the absolute values of aneurysm size have been used as a clinical variable when predicting the risk of aneurysm rupture, suggesting the possibility that other relevant factors may have been overlooked.1)2)13)16)18)25)27)
The behavior of the A com aneurysms was not reflected by the results from an international study on unruptured intracranial aneurysms (ISUIA). The results of ISUIA showed that aneurysms of < 7 mm in size and located in the A com were less likely to be discovered than aneurysms in other locations or of a larger size, thus increasing the likelihood of rupturing. More importantly, the results also provide statistical evidence that the A com aneurysms rupture even with smaller diameters than other aneurysms located elsewhere.2)15)16) Recently, the natural course of unruptured cerebral aneurysms in a Japanese cohort (UCAS Japan) has been presented in detail. In the referred study, aneurysms in the anterior and posterior A com were found to be more likely to rupture as compared to those in the middle cerebral artery. In particular, the A com aneurysms have been shown to rupture at a relatively high rate, even when they are < 7 mm in diameter.20)27) These results suggest that alternative factors-such as aneurysmal morphology-strongly correlate with the aneurysm rupture risk. Increasing evidence indicates that the relationship between the size of an aneurysm and aneurysm rupture may not be correlated.4)5)6)7)8)10)15)19)24)26)28)31)34)36)38)
The aim of the present study was to evaluate whether the A com aneurysms behave differently from the aneurysms located elsewhere with respect to size being a rupture risk. To this end, we examined the clinical data of ruptured A com aneurysms and analyzed other morphological parameters, including size parameter, providing adequate data for predicting rupture risk of the A com aneurysms.
MATERIALS AND METHODS
Patients
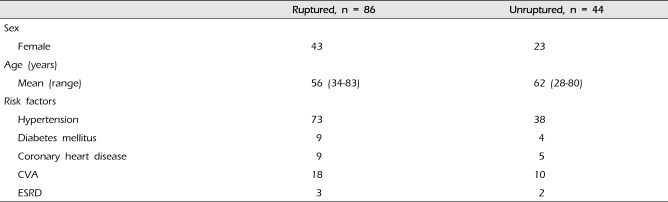
Between January 2010 and December 2015, a total of 130 consecutive patients at our institution with the A com aneurysms-86 ruptured and 44 unruptured-were included in this study. The ruptured group included 43 females (50%) and 43 males (50%) with the mean age of 56 years (range, 34-83 years). The unruptured group included 23 females (52%) and 21 makes (%) with the mean age of 62 years (range, 28-80 years) (Table 1). All patients underwent either digital subtraction angiography or 3-dimensional computed tomography angiography. The exclusion criteria for this study were the patients with fusiform, traumatic, or mycotic aneurysm. There were preexisting known risk factors, such as hypertension in 73 patients, who required antihypertensive medication; other risk factors included diabetes mellitus (9 patients), coronary heart disease (9 patients), previous cerebral stroke (18 patients), and end-stage renal disease (3 patients) in the ruptured group. In the unruptured group, 38 patients had hypertension, 4 had diabetes mellitus, 5 had coronary heart disease, 10 had a previous cerebral stroke, and 2 had end-stage renal disease.
Aneurysm characteristics
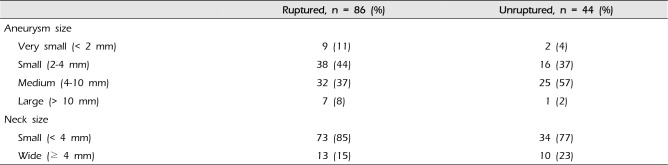
The ruptured group consisted of 9 very small (< 2 mm), 38 small (2-4 mm), 32 medium (4-10 mm), and 7 large (> 10 mm) aneurysms; the unruptured group consisted of 2 very small, 16 small, 25 medium, and one large aneurysms. There were 73 ruptured aneurysms with small necks and 13 with wide necks (neck size > 4 mm), and 34 unruptured aneurysms with small necks and 10 with wide necks (Table 2).
Morphological study of aneurysms
Seven morphological parameters were included in this study: the size of the A com artery, maximum size of aneurysm, width of aneurysm neck, morphology of aneurysm wall, size ratio, height/width ratio (aspect ratio), and difference of the dominant A1 artery. We measured the size of the A com (the maximum cross-sectional diameter of the A com artery), aneurysm height (maximal orthogonal distance from the dome to the neck), width (maximal diameter perpendicular to height) and neck width (the maximum diameter of the neck plane) for each aneurysm in the A com. The morphology aneurysm wall was evaluated as either smooth (a single regular pouch without protrusions) or irregular (with protrusions or secondary pouches). In addition, the bilateral A1 arteries (the maximum cross-sectional diameter of the A1 portion of the anterior cerebral artery) were measured. According to the method described in Dhar's report,10) the size ratio was defined as the ratio of the maximum aneurysm diameter to the average parent vessel diameter. The average parent vessel diameter was obtained by measuring two representative parent vessel cross sections. The height/width ratio (aspect ratio) was measured as the ratio of the maximum aneurysm height to the maximum diameter of width of aneurysm. By definition, a positive difference of the dominant A1 meant a difference of over 2 mm between the bilateral A1 portions of the anterior cerebral artery.
RESULTS
Morphological study
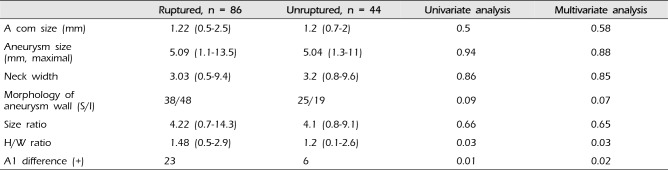
The results of morphological parameters of the A com aneurysms are summarized in Table 3. The mean size of the A com artery was 1.22 mm (range, 0.5-2.5 mm) in ruptured aneurysms and 1.2 mm (range, 0.7-2 mm) in unruptured aneurysms. In addition, the mean maximal size of the A com aneurysms was 5.09 mm (range, 1.1-13.5 mm) in ruptured aneurysms and 5.04 mm (range, 1.3-11 mm) in unruptured aneurysms. A statistical analysis revealed no significant difference in either the size of the A com artery (p = 0.63) or maximal size of the A com aneurysm (p = 0.82). All A com aneurysms included in the present study were of the saccular type with regard to their morphology. A smooth aneurysm wall was observed in 38 aneurysms(44%) in the ruptured group and 25 aneurysms (57%) in the unruptured group. An irregular wall was found in 48 ruptured aneurysms (56%) and 19 unruptured aneurysms (43%); a smooth wall was more frequently associated with unruptured than with ruptured aneurysms (57% vs. 44%). Conversely, an irregular wall was more frequently associated with ruptured than unruptured aneurysms (56% vs. 43%). However, the abovementioned differences between ruptured and unruptured aneurysms did not reach statistical significance (p = 0.09). The mean size ratio of the A com artery was 4.22 mm (range, 0.7-14.3 mm) in ruptured aneurysms and 4.1 mm (range, 0.8-9.1 mm) in unruptured aneurysms. The mean neck width of the A com aneurysm was 3.03 mm (range, 0.5-9.4 mm) in the ruptured group and 3.2 mm (range, 0.8-9.6 mm) in the unruptured group. These factors of trends did not reach statistical significance (size ratio, p = 0.66; neck width, p = 0.86). The mean height/width ratio (aspect ratio) of the A com aneurysm was 1.48 (range, 0.5-2.9 mm) in ruptured aneurysms, and 1.2 (range, 0.1-2.6 mm) in unruptured aneurysms (p = 0.03). The statistical analysis suggested that this difference between the two groups had a significant predictive value of aneurysm rupture. For all A com aneurysms included in this study, diameter of the bilateral A1 arteries were measured. The positive difference of the dominant A1 was observed in 23 ruptured aneurysms (27%) and 6 unruptured aneurysms (14%), with a statistical significance between the two groups (p = 0.01).
Risk factors
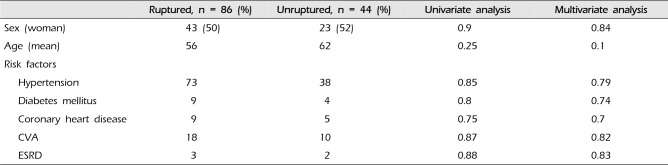
The results of risk factors associated with the A com aneurysms are summarized in Table 4. Risk factors, including hypertension, diabetes mellitus, coronary heart disease, a previous cerebral stroke, and end-stage renal disease, were not statistically significant for the prediction of rupture in both groups.
DISCUSSION
The prevailing view is that larger aneurysms have a greater risk of rupture. Predicting the risk of aneurysmal rupture, especially for aneurysms with a relatively small diameter, continues to be a topic of discourse. In fact, the majority of previous large-scale studies have used the maximum size of aneurysms as a predictor of aneurysm rupture.8)11)12)14)17)18)28)29)33)37)38) However, several investigators have attempted to find a better index or factors than the absolute maximum size of an aneurysm. It appears likely that some risk stratification of aneurysms must at some point involve a greater predictive power than the one affordable with aneurysm size alone.
As demonstrated by the results of the present study, the majority of ruptured A com aneurysms were smaller than 4 mm in size (55%). This indicates that the A com aneurysms may rupture despite their smaller size at the earlier stages of their development. Previous studies demonstrated that a large number of ruptured A com aneurysms had a size of < 5 mm.1)2)9)12)15)16)21)28)33)35)37) With regard to the discrepancy about the small size of ruptured aneurysms, which has been experienced in clinical practice, there are possible hypotheses explaining this discrepancy. Some authors have speculated that the size of an aneurysm may decrease after rupture.1)18) However, there has been no definite angiographic and histological evidence supporting this hypothesis. Using a collection of aneurysm measurements with pre- and post-rupture images, Rahman et al.31) reported that aneurysm size did not shrink. Conversely, other studies presented angiographic and histological evidence showing that aneurysms did shrink after rupture.1)12) Some previous studies suggested that most aneurysms that bleed do so shortly after formation; thus, they were never detected as unruptured aneurysms.9)33) Said differently, most acute subarachnoid hemorrhages result from recently formed aneurysms. After this initial period, the risk of rupture falls to a low level. Sonobe et al.33) suggested that most incidentally detected unruptured aneurysms have passed into the safe period with a low bleeding rate on the follow-up, whereas most ruptured small aneurysms were observed in the routine daily clinical practice. These findings are consistent with the very low risk of rupture associated with unruptured aneurysms and the small sizes of ruptured aneurysms that are encountered in clinical practice. It means a different type of aneurysm evolution from a rapid growth of an aneurysm and rupture at a small size within days or months to a slower growth with rupture occurring after years or remaining rupture-free for decades.
Aneurysms of the A com complex are more likely to have asymmetric A1 segments and to have asymmetric inflow angiographically from the hypoplastic A1 segment. The asymmetric nature of the A com artery results in the configuration of the A com aneurysms analogous to that of the terminal or bifurcation aneurysms. As such, there was the potential for the aneurysm to receive differing proportions of the parent artery inflows. This allowed us to consider the hemodynamics for the A com artery aneurysms rupture. Weir et al.37) analyzed the difference of the dominance of A1 arteries between ruptured and unruptured aneurysms. They reported that, given their study population, 35% of ruptured aneurysms were the A com aneurysms, whereas only 11.2% of unruptured aneurysms were of this type. Other previously published data related to unruptured intracranial aneurysms also demonstrated 10% to 15% of unruptured aneurysms to be the A com aneurysms.16) These data are consistent with the results of our study. This phenomenon implies that midline lesions like the A com aneurysms are at a greater risk of rupture, although their size is smaller than that of more laterally situated aneurysms. Carter et al.3) explained that aneurysms arising from smaller vessels tend to be small and unstable, because they have thinner walls as compared to the aneurysms originating from a large artery. Therefore, it is suggested that rupture risk of an unruptured aneurysm is related to the location of that aneurysm and the parent vessel diameter. In addition, Ohashi et al.28) reported that the diameter of the A com aneurysm and the distal anterior cerebral artery is smaller than that of the middle cerebral artery and the internal carotid artery. Thus, aneurysms located in the A com may bleed before reaching a larger size.
The A com artery is known to be one of the common sites of aneurysm rupture. Given the diversity of geometry, the difference of the dominance of A1 arteries, and flow dynamic conditions, the A com is considered to be the most complex in the anterior circulation of the cerebral artery. Aneurysmal morphology may be an important factor related to rupture. Many morphological parameters, such as the size ratio, 10)20)23)24)31)36) height/width ratio (aspect ratio),15)22) bottleneck factor,15) and aneurysm volume and surface area,30) have been suggested as very simple factors that provide useful information to determining relevant treatment and follow-up strategies for patients. Concurrently, these parameters also provide an effective means to evaluate the risk of rupture for aneurysms. Morphological parameters represented, resulting in more complex intra-aneurysmal flow patterns, multiple vortices, and low aneurysmal wall shear stress.10)20)24)31)36) There is no simple cut-point value for any of the aneurysm-related parameters that would divide unruptured aneurysms into those that need to be treated actively and those that should be left untouched. The evidence, from all reports on risk factors for aneurysm rupture, is still insufficient to characterize exactly which aneurysms will certainly rupture. In our study, as concerns the aneurysm rupture risk, height/width ratio and the difference of the dominant A1 artery were correlated with aneurysm rupture. In terms of height/width ratio, these results could be related to more ruptured aneurysms with small impaction zones, higher inflows, and, consequently, a higher wall shear stress (jet inflow).5)32)39) Aneurysms in the A com complex are more likely to have asymmetric A1 segments and to have asymmetric inflow angiographically from the hypoplastic A1 segment. The result of the asymmetric nature of the A com is that many aneurysms are configured analogously to terminal or bifurcation aneurysms. As such, there was the potential for aneurysms to receive differing proportions of the parent artery inflows. This allowed us to consider the hemodynamics for the A com aneurysms rupture.
This study has several limitations. First, our study had an insufficient number of cases to definitively conclude the predictability of rupture risk of the A com aneurysms. A better understanding may be possible through a multicenter, population-based study (transverse study); in addition, cost and ethical issues preclude screening for aneurysm in a randomly selected population. Second, in our study, no statistically significant differences were found between ruptured and unruptured aneurysms with respect to age, gender, and risk factors, such as hypertension, diabetes mellitus, coronary heart disease, a previous cerebral stroke, and end-stage renal disease. Several previous studies have analyzed the predictive factors for aneurysmal ruptures.16)17)18)33)38) They concluded that a history of cerebral stroke, multiple aneurysms, younger patient age, hypertension, and smoking are risk factors. However, the risk factors identified in our study are not consistent with the results of previous publications. It might be caused by the bias of compounding variables, comparing between ruptured and unruptured aneurysms in terms of the overall clinical or premorbid risk factors, such as age, history of hypertension, smoking, and genetic predisposition. These should be considered to provide a more comprehensive picture of the differences between ruptured and unruptured aneurysms.
CONCLUSION
Through a comparison of morphologies and an analysis of the A com aneurysms with a trend of differences between the ruptured and unruptured groups, the A com aneurysm may rupture despite their smaller sizes. In addition, the morphology parameter of height/width ratio and difference of the dominance of A1 may be useful for describing aneurysm risk of rupture. Further studies are needed to integrate all this information and help clinicians provide individualized recommendations to patients and the general population. To reconcile these findings with the prediction of the A com aneurysms, a definitive understanding of these aneurysms through a large, multicenter, collaborative study, in a prospective manner, is required. In addition, new tools are being developed to assess the risk of rupture using embryogenesis, blood flow coherence, genetics, and hemodynamic evaluation. Finally, new treatments are required as well, which could be furthered by a definitive understanding of aneurysms.
 XML Download
XML Download