

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Subarachnoid hemorrhage (SAH) due to a solitary spinal aneurysm is extremely rare, representing less than 1% of all cases of SAH reported in the literature. Aneurysms involving the radiculomedullary arteries are particularly rare, with only nine cases previously reported.1)2)3)6)11)12)14)16) The most common etiology of spinal SAH is spinal arteriovenous malformations (AVM); other etiologies include arterial dissection, neoplasm, moyamoya disease, systemic lupus erythematosus, and Behçet disease (BD).12)14) Various etiologies can contribute to the development of spinal artery aneurysm. The purpose of this case report is to describe the successful surgical treatment of a ruptured aneurysm in the radiculomedullary artery in a patient with BD.
CASE REPORT
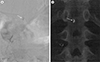
A 49-year-old man with BD presented to our outpatient department with a 3-month history of severe lower abdomen and leg pain, with no history of trauma. The patient had a medical history of hypertension, uveitis, and oral ulcer, with use of appropriate medications for these conditions. His erythrocyte sedimentation rate (ESR) was 30 mm/h. Neurological examination revealed hyperesthesia below the level of T12 and an increased deep tendon patellar reflex, bilaterally. Magnetic resonance imaging of the lumbar spine revealed a 3 mm enhanced intradural-extramedullary mass at the T12 level with extensive SAH and cord compression due to hematoma (Fig. 1). Spinal angiogram was performed for further diagnosis of the suspected vascular lesion at T12. Selective injection into the right L2 segmental artery revealed a 5.5 × 3.2 mm intradural aneurysm receiving direct blood supply from the radiculomedullary artery at the T12 level (Fig. 2). The Adamkiewicz artery was visualized on left T9 segmental artery angiogram and the anterior spinal artery (ASA) was visualized below the L2 level communicating with this artery. Based on our findings, we chose to perform surgical resection.
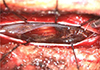
Laminectomy was performed from T10 to L2. After opening the dura, diffuse SAH was found and the hematoma was thick, resulting in spinal cord compression. After removal of the hematoma, the ruptured aneurysm was exposed. Active bleeding persisted as we explored the aneurysm and we identified a dissecting lesion at the distal section of the aneurysm (Fig. 3). Temporary clips were applied to the parent arteries; we then evaluated for changes in neurophysiological monitoring to identify whether complete resection would lead to ischemic complications. During the five minutes of temporary clipping, no abnormalities were detected on neurophysiological monitoring; thus, the aneurysm was completely resected.
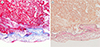
Pathological examination of the surgical specimen revealed a degenerated vascular wall with thrombus, suggestive of an aneurysm wall without inflammatory cell infiltration (Fig. 4). No surgery-related complications were identified and the patient recovered fully after the surgery.
DISCUSSION
Aneurysms of the radiculomedullary artery are extremely rare, with nine cases identified in the literature, as summarized in Table 1.1)2)3)6)11)12)14)16) To our knowledge, this is the first case report of a ruptured aneurysm of the radiculomedullary artery, which was surgically treated in a patient with BD.
Aneurysm associated with spinal AVM is the most common cause of spinal SAH.12)13) Other known conditions associated with spinal aneurysm include arterial dissection, neoplasm, BD, systemic lupus erythematosus, moyamoya disease, fibromuscular dysplasia, pregnancy and infection.1)2)3)4)5)6)7)8)9)11)12)13)14)16) BD is a type of systemic vasculitis that primarily affects the eyes, skin, joints, blood vessels, and nervous system.10)15) Vascular involvement is not uncommon with BD, with a reported prevalence ranging between 7% and 29% of all cases.15) Although the venous system is involved in most cases, arterial aneurysms are a leading cause of death in this clinical population. When present, arterial aneurysms typically expand rapidly and result in fatal rupture. When present in patients in BD, aneurysms most commonly develop in the aorta, and the femoral or pulmonary arteries, with involvement of branch arteries being uncommon. Spinal SAH due to ruptured solitary spinal artery aneurysm is extremely rare in BD.1) We found only one reported case, a patient with ruptured radiculomedullary artery aneurysm at the C5 level. In our case, based on the identification of a dissecting lesion at the distal section of the aneurysm during surgery and no evidence of inflammatory cell infiltration on pathological examination (which are specific finding of aneurysm associated with BD), we hypothesized that dissection of the aneurysm was the primary event, resulting in the formation of a pseudoaneurysm with subsequent hemorrhage.
The symptoms of ruptured spinal aneurysm seem to correlate with the level of the lesion. Ruptured aneurysm at the cervical level can cause meningeal irritation due to intracranial SAH or quadriparesis. Lesions involving the thoracolumbar levels can cause lower back pain, abdominal pain, and motor weakness or sensory changes of the lower extremities. Our patient complained of back pain and sensory changes of the lower extremities. These symptoms were suggestive of aneurysm at the thoracolumbar levels and the lesion was identified at the T12 level.
There is no standard treatment guideline for ruptured spinal aneurysms because these lesions are very rare. Therefore, the choice of proper treatment, including surgery, endovascular embolization, and conservative treatment, remains controversial. Conservative therapy has been preferred in cases of small ruptured dissected aneurysms at the ASA or Adamkiewicz artery which must be preserved to reduce neurological complications, and solitary aneurysms associated with underlying disease, such as BD, which can show spontaneous healing of the dissected aneurysms with patent flow.1)2)6) Endovascular treatment can be a treatment option if the surgical procedure is difficult due to the location of the lesion or the patient's general condition.8) However, because most spinal artery aneurysms are fusiform rather than saccular shape and endovascular treatment has the potential risk of causing vascular injury or thrombosis that could lead a poor neurological outcome, endovascular treatment is usually not an option.2) Surgery may be an appropriate choice for the ruptured spinal artery aneurysms, especially if the distal flow is absent or the surrounding hematoma produces a mass effect on the spinal cord. If no distal flow is confirmed on spinal angiogram, complete obliteration of the lesion can be performed to reduce the risk of re-bleeding. On the other hand, if distal flow is identified on spinal angiogram, wrapping can be an alternative treatment option that preserves the distal flow. In our case, the Adamkiewicz artery was identified on left T9 segmental artery angiogram and ASA flow was detected below the L2 level. We assumed that although the ruptured dissecting aneurysm was surgically resected, blood flow from Adamkiewicz artery to the ASA was sufficient to supply the lower L2 level. In addition, to enhance safety of the surgery, we also evaluated neurophysiological monitoring results during temporary clipping of radiculomedullary artery and during the entire procedure. There was no change in neurophysiological monitoring, and we could thus completely resect the aneurysm.
Based on our experience in this case, we propose that surgical treatment of a ruptured radiculomedullary artery aneurysm with collateral flow from the Adamkiewicz artery is feasible with application of a careful surgical technique, including temporary clipping and intraoperative neurophysiological monitoring, to achieve a good clinical outcome.
CONCLUSION
Ruptured spinal aneurysm of the radiculomedullary artery is a rare vascular lesion. With only nine cases previously reported, it is difficult to define an optimal treatment approach. However, based on our experience, we propose that early surgical resection of this aneurysm by careful surgical technique, including temporary clipping of the parent artery and intraoperative neurophysiological monitoring, when the Adamkiewicz artery is identified near the lesion, might be effective in preventing cord ischemia and improving neurological outcome.


 XML Download
XML Download