

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With the coming up of endovascular coiling as a standard therapy for treatment of cerebral aneurysms, complications that are related to it are also coming up. Distal migration of the coil is one of the serious complications. If not managed quickly, it can lead to thrombus formation and vessel occlusion resulting into cerebral infarction.
CASE REPORT 1
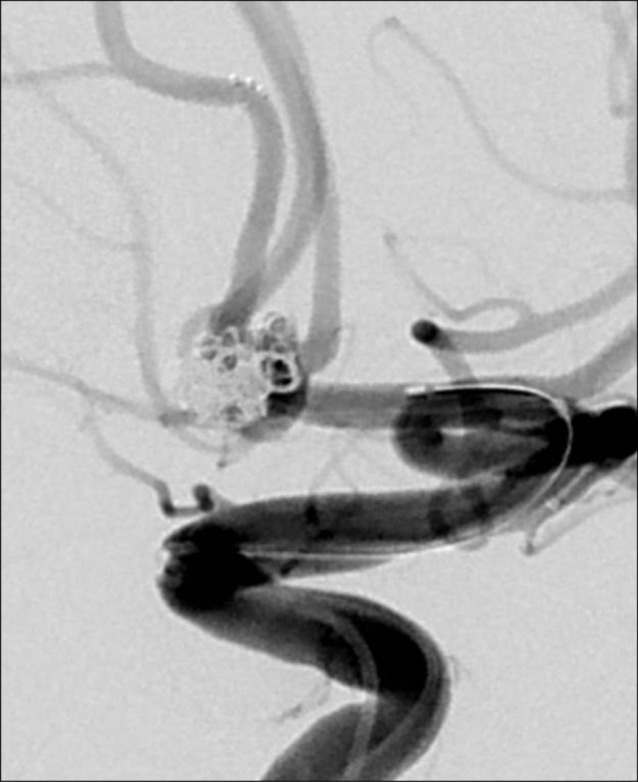
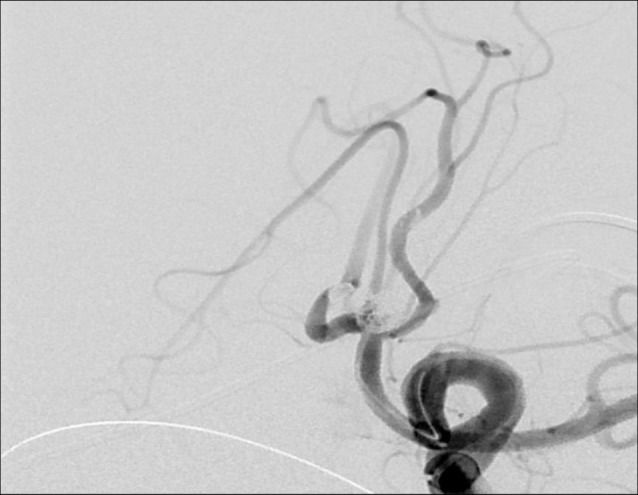
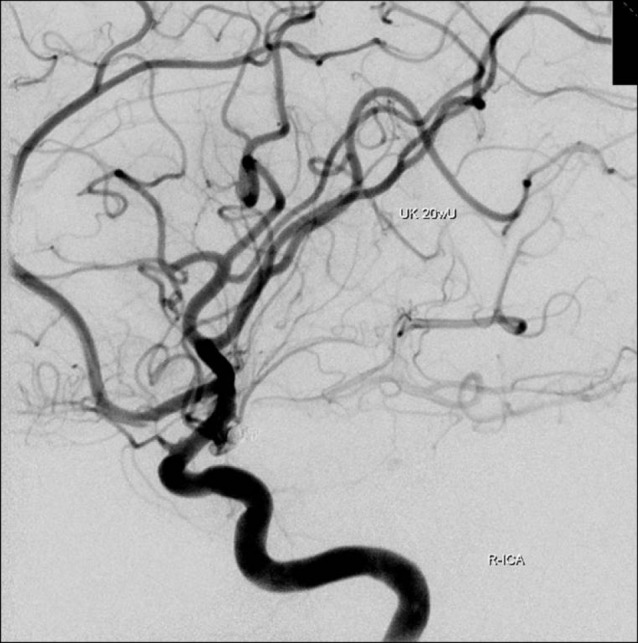
A 57-year-old woman underwent balloon assisted coil embolization, for ruptured anterior communicating (A-com.) aneurysm. Her angiogram one year later showed residual aneurysmal sac (Fig. 1).
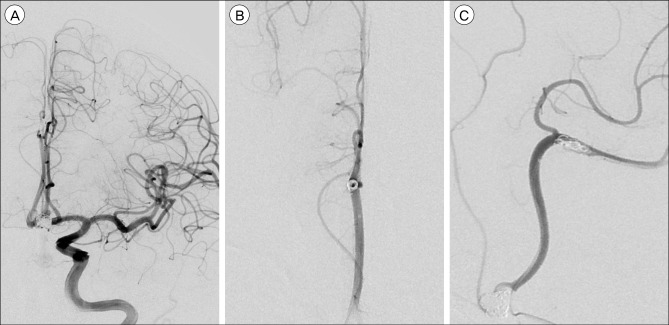
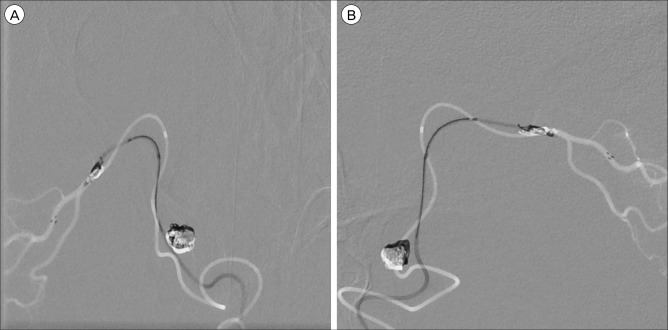
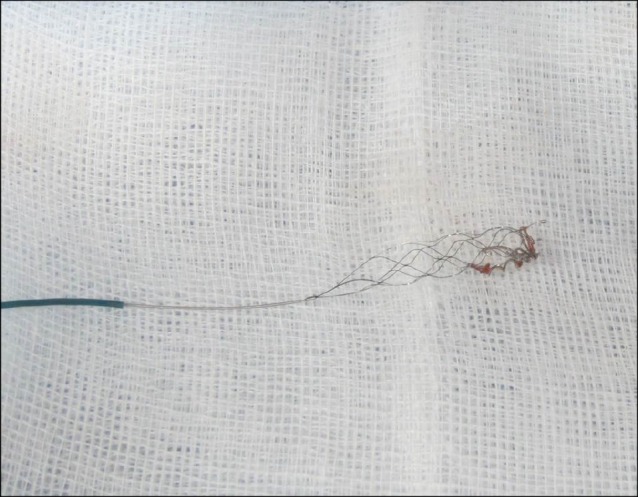
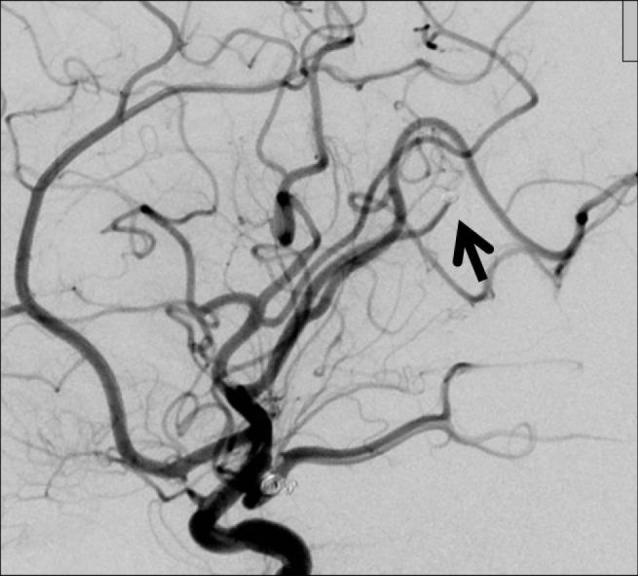
Stent-assisted coiling of the remnant sac was planned (Fig. 2). 75 mg of clopidogrel and 100 mg of aspirin was given for 5 days before the procedure. During the procedure a coil (MicroPlex HyperSoft Helical 1.5 × 1 mm, Microvention, Tustin, CA, USA) migrated into the contralateral anterior cerebral artery (ACA) (Fig. 3). Initially it got lodged into the right A2 segment but it migrated further and finally it got lodged into the distal callosomarginal artery (Fig. 4), causing its occlusion. We removed undetached stent, and a microcatheter (Prowler Plus Select, Codman Neurovascular, Raynham, MA, USA), which was initially used for stent-assistance, was negotiated beyond the occluded ACA (Fig. 5), and Solitaire® AB 4 × 15 mm stent was passed through it distal to the occluded artery and was deployed (Fig. 6). It was then gradually withdrawn, entangling the migrated coil and was captured into the microcatheter. Microcatater along with the stent was then withdrawn, retrieving the displaced coil along with it (Fig. 7).
CASE REPORT 2
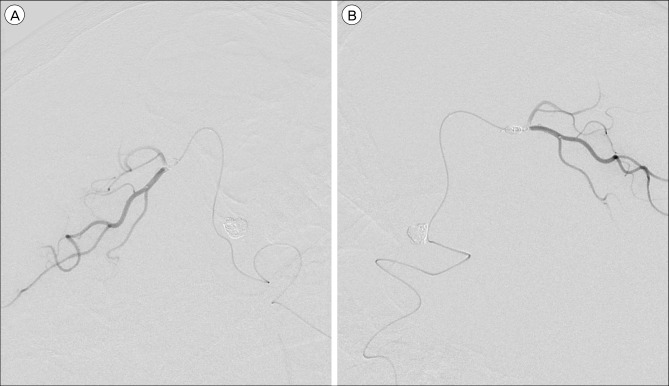
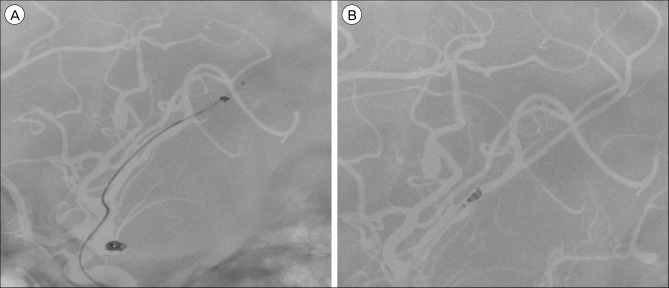
A 44-year-old female presented with SAH, Hunt and Hess grade 2. Her cerebral angiogram showed the right posterior communicating (P-com.) artery aneurysm, sized 2.2 × 2.2 × 6.1 mm (Fig. 8). After placement of 3 coils, there was still some space remning near the neck. A DeltaPlush (Codman Neurovascular, Raynham, MA, USA) 1.5 × 2 mm coil was used to pack the sac. After the coil was detached it got dislodged from the aneurysm and migrated into the right MCA branch (Fig. 9). A microcatheter (Rebar18, Covidien, Irvine, CA, USA) was passed beyond the embolic coil and a 4 × 15 mm sized Solitaire® Stent was passed through it distal to the migrated coil. The stent was then, successfully withdrawn along with the microcatheter retrieving the entangled coil along with it (Fig. 10, 11).
DISCUSSION
Coil migration is a well-known complication associated with endovascular coiling. It can cause brain ischemia due to distal vessel occlusion. Factor that predispose to this complication are wide neck aneurysms, small fundus to neck ratio, tortuous vessel, unstable microcatheter position, use of undersized coil, premature detachment and high flow conditions. Despite continual improvements in materials and techniques, the risk of coil misplacement or migration, even in the hands of experienced and skilled operators, remains.
Various strategies to remove displaced coils have been reported,1)2)3)4)5)6)7)8)9)10)11)12)14)16)17)19)20)21) including surgery,15)18) but none of them appears easy and reliable.
Already 2 cases of coil retrieval using a Solitaire® stent have been reported in the English literature.5)9)
In this case report, we have presented two cases in which there was an accidental coil migration during aneurysmal coiling. In both the cases Solitaire® AB stent was successfully used to retrieve the distally migrated coil. The Stent was carried distal to the migrated coil and was expanded. The expanded stent was then gradually withdrawn, leading to the entangling of the migrated coil into the struts of the stent. The Stent was then withdrawn along with the migrated coil.
Initially the Solitaire® stent, which is a self-expanding and fully retrievable even after full deployment, was developed and designed as neurovascular reconstruction device for endovascular treatment of wide-necked and complex intracranial aneurysms. But, nowadays due to its peculiar structural design, it is also used for mechanical thrombectomy.13)
We found that the Solitaire® AB stent can be used to retrieve distally migrated coil in vessels of small diameter where the use of other devices can be dangerous or technically demanding. Owing to its Parametric™ design (an overlapping stent-based technology), its struts can overlap, at least partially, when the stent is compressed. These overlapping struts allow the stent to be crimped to a smaller initial delivery diameter than may be achieved with non-overlapping designs for given metal density. This reduces the delivery diameter which allows the stent to be placed in the distal small tortuous vessels and thus it can be safely used to retrieve coils that have migrated to distal vessels, which may not be possible with other alternatives.
Problems that have been associated with coil retrieving devices are lack of universal availability, complications associated with them, and most importantly, because they are very infrequently used, they could be difficult to handle.
Micro-snare and Merci Retriever (Stryker; Kalamazoo, MI, USA), especially when used in small diameter vessels can cause vessel wall injury,3)4)16) Although we have used Solitaire® stent for coil retrieval in only two cases we did not face any problem using it. But we think that the complications that could be associated with it would not be different from those that are encountered, when it is used for mechanical thrombolysis and there, it has been found to be having low complication rate.
Because of its frequent uses, such as vascular reconstruction for aneurysm coiling and mechanical thrombectomy, Solitaire® stent is readily available is easy to handle as compared to other devices.
Although using a Solitaire® stent for retrieval of distally migrated coils is off-label use, the technique with a Solitaire® stent provides us a simple and safe method to retrieve the distally migrated coil, especially for the coils that get lodged in distal small vessels. It has one more advantage of universal availability. Therefore, it could be considered as an option for removing migrated coils.


 XML Download
XML Download