

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Spinal artery aneurysms are most commonly associated with high-flow states secondary to either arteriovenous shunting or occlusive disease of larger arteries causing increased flow through spinal arteries recruited as collateral circulation.1)2)4) An aneurysm is considered "isolated" when it occurs in the absence of such a high flow state. Aneurysms of the spinal vasculature are more common along the anterior axis than the posterior axis, and isolated aneurysms account for only a small fraction of these. Histologically, isolated spinal artery aneurysms have features shared with cerebral artery aneurysms,7) suggesting that at least some may be the product of a congenital predisposition to aneurysm formation. However, isolated anterior spinal artery and cerebral artery aneurysms have been associated with both central nervous system-specific and systemic vasculitis.5)13)17)20) Here, we present the first case to our knowledge documenting a posterior spinal artery (PSA) aneurysm in the context of a hypersensitivity vasculitis (leukocytoclastic vasculitis).
Go to : 
CASE REPORT
History and presentation
A 53-year-old male with a history of hepatitis C, hepatitis B, and poly-substance abuse presented to an outside hospital for bilateral lower-extremity recurrent cellulitis, hypoalbuminemia and acute kidney injury. On the ninth day of admission, the patient developed acute paraplegia associated with a T5/6 sensory level deficit. A thoracic spine magnetic resonance imaging (MRI) obtained on the day of presentation was read as negative for evidence of compressive cord lesion and the patient was medically managed with broad-spectrum antibiotics and steroids.
The patient's neurological symptoms did not improve with medical management and 15 days later a second thoracic spine MRI was obtained. A hyper-intense intradural lesion was noted (Fig. 1A) with compressive effects at the level of C7-T1 with associated increase in T2 signal intensity in the cord extending from C7-T5, suggesting edema. The patient was subsequently transferred to our institution for further evaluation. Thoracic spinal angiography revealed a 1.5 mm ectasia of the right T9 segmental artery's radiculopial branch, consistent with an aneurysm of the posterior spinal artery (Fig. 1B). In addition to the right T9 aneurysm, a segment of the left T5 radiculopial artery revealed vascular pathology along the posterior aspect of the spinal cord suggestive of either an inflammatory process or post-hemorrhagic reactive changes (Fig. 1C). Vascular bleeding and lumen irregularities consistent with an acute inflammatory process were noted throughout the cervical and thoracic spine, and the angiogram also revealed a 3 mm right middle cerebral artery (MCA) aneurysm.
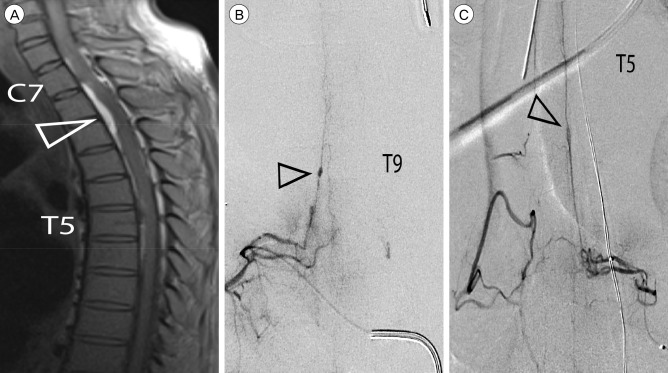 | Fig. 1Diagnostic imaging, 15 days (MR) and 16 days (Angiography) post-presentation. (A) Sagittal T1 MR with compressive hyper-intense ventral lesion at T2-level (open arrowhead) and axial extension from C7-T8. (B) Masked angiogram of the T9 radiculopial artery with 1.5mm ectasia (open arrowhead). (C) Masked angiogram of the T5 radiculopial artery with lesion suspicious for vascular pathology (open arrowhead).
|
Intervention
A coil was placed in the segmental artery supplying the T9 aneurysm for subsequent intra-operative localization during the open resection. The patient underwent a multilevel laminectomy (C7-T2 and T8-10) for hematoma evacuation and microsurgical aneurysm resection. The lesion at T9 (Fig. 2A) was resected and submitted to pathology. The histology was consistent with a dissecting aneurysm with localized regions of lymphocytic infiltration of the intima, and fibrosis and necrotic changes in regions of the tunica media (Fig. 2B, C). No histological abnormalities were noted in the adjacent, non-aneurysmal vessel wall. Samples of the hematoma from the T2-level had histological features consistent with an organizing intradural hematoma. He was returned to the medical service on post-operative day 2.
 | Fig. 2Intraoperative images and photomicrographs stained with hematoxylin and eosin. (A) Intraoperative image of the aneurysm in situ with the T9 nerve root retracted. (B) Adjacent segments of the parent vessel wall appear normal (filled arrowhead) compared to the aneurysm wall (open arrowhead; 100 ×). (C) Myxoid degeneration (open arrowhead) and medial necrosis with fibrin deposition (filled arrowhead), both typical features of an aneurysm, were present in the aneurysm wall (400 ×).
|
Postoperative course
Multiple medical issues complicated the postoperative course. Neurologically, the patient's pre-operative deficits remained unchanged for the duration of his hospitalization. Medically, the patient deteriorated over the next 60 days. He developed anuric renal failure and hypercapnic respiratory distress. Rheumatologic work-up revealed low C3 and C4 levels. A skin biopsy was performed which was positive for leukocytoclastic vasculitis. Renal biopsy demonstrated membranoproliferative glomerulonephritis secondary to hepatitis C virus-related cryoglobulinemic vasculitis and he underwent treatment with rituximab, plasmapheresis and prednisone with improvement in his renal function. The patient subsequently developed a urinary tract infection with multiple-drug resistant Klebsiella and was started on imipenem. Several days later the patient became hypoxic and hypotensive. The family declined further interventions, and the patient expired.
Go to :
DISCUSSION
Very little is known about the pathophysiology of isolated PSA aneurysms. Here, we present the case of a ruptured PSA aneurysm in the context of a leukocytoclastic vasculitis. Spinal angiography demonstrated evidence of diffuse inflammatory process affecting multiple levels, histology confirmed the presence of a leukocytic infiltrate at the site of the resected aneurysm and subsequent skin biopsy confirmed the diagnosis of leukocytoclastic vasculitis. Leukocytoclastic vasculitis is a small-vessel hypersensitivity vasculitis resulting from immune complex deposition in the vessel wall, leading to lymphocytic infiltration. This inflammatory process may have predisposed our patient to aneurysm formation, or it may have compromised the wall integrity of a pre-existing PSA aneurysm, precipitating rupture. We identified 14 cases of isolated PSA aneurysms, which are summarized in Table 1. None occurred in the context of a confirmed vasculitis but it is not clear that vasculitis was ruled out. For the current case, an important question remains whether diagnosis and treatment of the vasculitis could have prevented aneurysm rupture.
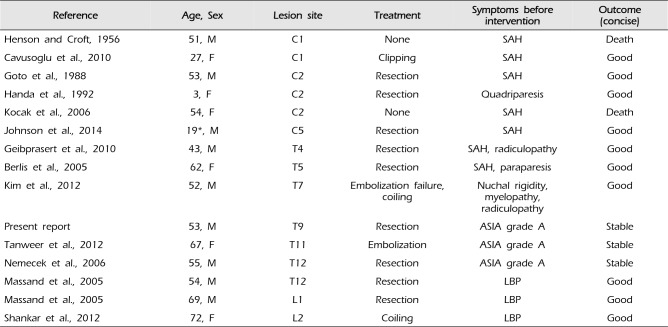
Table 1
Literature review of isolated PSA aneurysms
![]()
The natural history of spinal aneurysms likely mirrors that of intracranial aneurysms, although published natural history data of spinal aneurysms is sparse. Most presented after an initial rupture and rehemorrhage occurred in 2 of 15 cases (13%). The average age at presentation was 48.6 (95% confidence interval: 37.8-59.5) years. When cervical and thoracolumbar lesions were considered separately, cervical lesions tended to present at a younger age (Fig. 3A). Three of 15 patients (20%) exhibited multiple aneurysms; 2 of the 14 reported cases harbored other spinal artery aneurysms,14) while our patient had an additional MCA artery aneurysm. This rate is similar to the rate of multiple aneurysms observed in patients with cerebrovascular aneurysms, where 20-30% of patients with at least one cerebrovascular aneurysm will have multiple aneurysms.19) Our analysis of the limited data available is consistent with the assumption that PSA aneurysms and cerebral aneurysms share similar epidemiology, natural history and re-hemorrhage risk.
 | Fig. 3Literature review on posterior spinal artery (PSA) aneurysm presentation, management and outcomes. (A) Age of presentation for cervical and thoracolumbar PSA aneurysms. (B) Outcomes observed in cases of cervical and thoracolumbar PSA aneurysms. Outcomes observed were not significantly different between cervical and thoracolumbar lesions (p > 0.5, Fisher's Exact test). (C) Cases that presented with pain or meningitic symptoms ("SAH") had significantly better outcomes after intervention than those that presented with symptoms of cord compression (p < 0.05, Fisher's Exact test). SAH = subarachnoid hemorrhage.
|
The clinical presentation of ruptured PSA aneurysms depends on the level of the lesion. Eighty-three percent of cervical-level PSA aneurysms present with signs and symptoms of intracranial SAH, including severe headache, nuchal rigidity, and nausea and vomiting in the absence of myelopathy. For infra-cervical PSA aneurysms, the presentation is more suggestive of spinal SAH (myelopathy, localized back pain, and radicular pain). Cervical lesions are more likely to present suddenly than infra-cervical lesions (66% vs. 33%, respectively). In summary, ruptured cervical PSA aneurysms are more likely to present in younger patients with symptoms of intracranial SAH (including blood in the basal cisterns) without any recent history of progressive symptom. In contrast, ruptured infra-cervical PSA aneurysms presented in older patients with symptoms of spinal SAH and a one-week history of lower back or abdominal pain.
Once identified, PSA aneurysms are amenable to resection, endovascular intervention, or watchful waiting. For ruptured PSA aneurysms, our literature analysis suggests that more aggressive management should be considered for cervical PSA aneurysms, as the only reported deaths have followed re-hemorrhage in these lesions prior to intervention. Indeed, the mortality rate of cervical lesions is higher than that of thoracolumbar lesions (33% vs. 0% mortality; Fig. 3B). Treatment modalities include either microsurgical resection or endovascular embolization. While newer microcatheters have made it possible to embolize these lesions, surgeons have historically chosen resection because the operation is curative and the superficial nature of the PSA aneurysm facilitates an open surgical approach. In addition, surgical decompression with a laminectomy can relieve compression caused by a hematoma. However, outcome is independent of approach (endovascular vs. open). Of patients who underwent intervention, those presenting with pain or meningitic symptoms were significantly more likely to have a positive outcome than those who presented with symptoms of cord compression (100% vs. 40% improvement; Fig. 3C). Thus, outcome now appears more dependent on symptoms at presentation, leaving the physican to choose intervention based on case-specific factors and personal preference.
For the present case, endovascular intervention was not pursued because occlusion of the proximal segmental vessel of the T9 aneurysm would not provide definitive cure, and there was concern that direct liquid embolic injection could result in additional spinal cord infarction. Since the patient required an evacuation of his hematoma to decompress his spinal cord, we felt that the aneurysm could be resected surgically at the same time and would provide a tissue sample to help establish a diagnosis for his suspected systemic vasculitis. Postoperatively, the patient was neurologically stable with negligible evidence of recovery. However, the patient's postoperative course was complicated by medical factors that resulted in the death of the patient after a protracted hospital course.
Go to :
CONCLUSION
In general, isolated PSA aneurysms are difficult to diagnose but are amenable to surgical intervention with good results. Cervical lesions have a higher mortality than thoracolumbar lesions, providing justification for more aggressive management. Patients who present with pain or meningitic symptoms are more likely to recover than those who present with symptoms of cord compression, a trend consistent with the results of the presented case. Once diagnosed, both open and endovascular approaches have been used successfully with high cure rates and low morbidity. Consequently, the choice of management strategy will ultimately depend on the specific anatomic pathology, the medical status of the patient, the patient's personal preference and the surgeon.
Go to :
 XML Download
XML Download