

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cerebral air embolism is known to be a harmful event affecting deep-sea divers. It can also occur iatrogenically during invasive medical procedures. Although infrequent, it has been steadily reported. Most of the reported cerebral arterial air embolisms (CAAE) are paradoxical transvenous embolism, but trans-arterial CAAE has also been reported occasionally.6)10)11)14) The mainstay treatment of CAAE is considered hyperbaric oxygen (HBO) therapy.2) However, HBO therapy does not always mean improvement. This report introduces two cases of CAAE that occurred during cerebral angiography, which improved without HBO therapy, and discusses the factors that influence air embolus absorption with the literature review.
CASE REPORT
Case 1
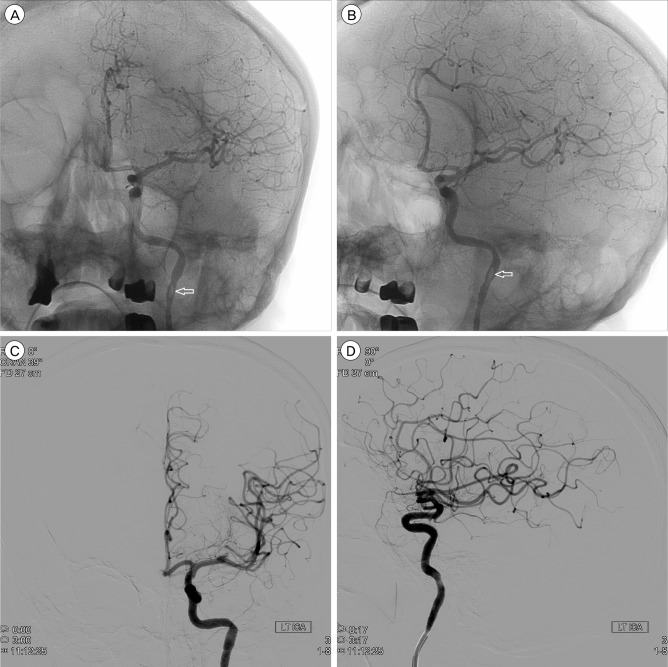
A 65-year-old man presented with vertigo. The cerebral magnetic resonance angiography revealed an unruptured aneurysm in the left middle cerebral artery bifurcation. Coil embolization was performed under general anesthesia. With the first rotational image acquired during the operation, we detected an air embolus at the distal end of the guiding catheter in the left internal carotid artery (ICA) (Fig. 1A). The air embolus migrated distally along the middle cerebral artery (Fig. 1B). During the migration, the embolus decreased in size and can be traced to the distal M2 segment of the middle cerebral artery. We detected no arterial occlusion from the angiograms taken immediately after the event (Fig. 1C, D). This air embolus disappeared spontaneously in a very short time. The embolization of the aneurysm was performed successfully, and the patient recovered from the anesthesia without any subsequent neurological complications.
Case 2
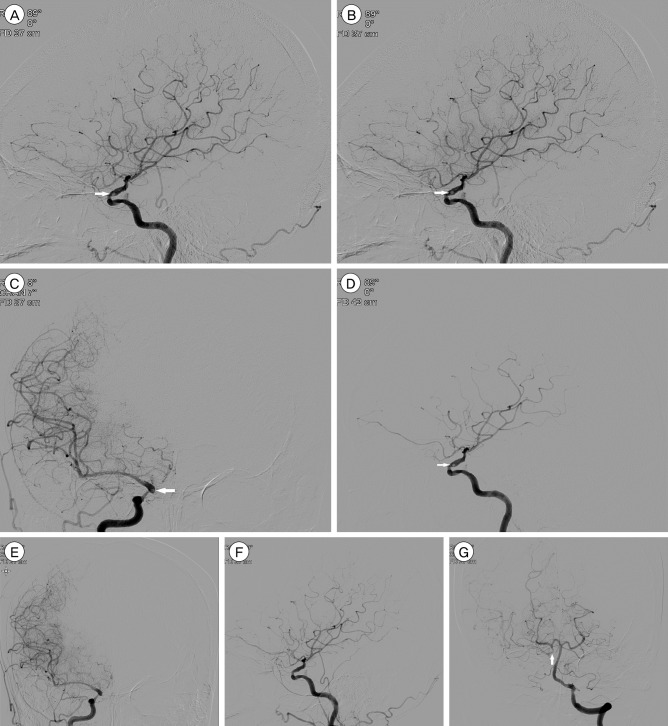
An 82-year-old woman visited our hospital because of left lower extremity weakness. She was diagnosed with severe right distal ICA stenosis and right internal border zone infarction from another hospital, 7 days prior. Transfemoral cerebral angiography showed 84% severe stenosis of the right supraclinoid ICA and prominent collateral flow to the ipsilateral middle cerebral artery via the right posterior communicating artery (Fig. 2A, G). A small air embolus was found in the supraclinoid ICA immediately after the first injection of right ICA angiography. It did not migrate distally, but was wandering in the supraclinoid ICA proximal to the posterior communicating artery (Fig. 2A, B and C). On the following angiography, the air embolus decreased in size, but remained wandering at the same site after 3 minutes (Fig. 2D). We could not find the air embolus in the supraclinoid ICA and the distal cerebral vasculature 27 minutes after the event on the following angiography (Fig. 2E, F). The patient showed no neurological abnormality after the angiography.
DISCUSSION
Based on reported literatures, the CAAE has occurred iatrogenically during various clinical procedures. Most of the CAAEs occur paradoxically, with air entering the vein during different medical procedures and moving into the arterial circulation through various arteriovenous fistulas.3)8)13) The trans-arterial CAAE during the cerebral angiography has been reported steadily, like in these cases.6)12)14)
Although the treatment of CAAE has not been established, HBO therapy is considered the primary treatment.2) However, HBO therapy has not always improved patients with CAAE; some patients treated with HBO therapy have neurological sequelae or even died. In contrast, some patients improved without HBO therapy.6)11)12)13) Two patients without HBO therapy also had no neurological abnormality in this report.
According to Henry's law, the amount of dissolved gas, such as oxygen and nitrogen, is influenced by its partial pressure and temperature. The fact that HBO therapy does not always coincide with a patient's results means that other factors affect air embolus absorption besides the partial pressure of gas, when the body temperatures are assumed not significantly different. Many factors are postulated in the literatures such as the volume of air in the artery, air delivery rates, entry route of air and HBO therapy onset.1)3)11)15)
The two CAAE cases in this report occurred during angiography, and the measured emboli diameters were 1.75 × 5.4 mm (52 µL) and 1.74 mm (22 µL). The first case showed the entire process of air embolus disappearance while migrating distally in the blood stream. The embolus in the second case was wandering in the supraclinoid internal carotid artery, gradually decreased in size, and was finally absorbed. The emboli sizes in our cases were relatively smaller than those reported in the literature.4)5)7)9) The small emboli can be absorbed in the atmospheric condition, not under hyperbaric environment, like in the present cases. As long as the embolus is smaller than the arterial lumen diameter, as seen in our two cases, it will gradually dissolve while migrating or wandering through the blood stream.
Case 1 showed the completed process in real time, wherein the air embolus from the guide catheter gradually decreased in size and disappeared from the middle cerebral artery M3 segment while migrating distally. This may be the first case that shows the entire absorption process of an air embolus on the moving image.
CONCLUSION
Some of the CAAE can be improved spontaneously without HBO therapy like in these cases; hence, we can expect that other factors such as embolus size besides pressure and temperature might affect improvement (of CAAE). Our cases demonstrating the dissolution of an air embolus in the blood stream provide a clue on factors affecting the dissolution.
 XML Download
XML Download