

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cerebral concussion is a mild head trauma that occurs commonly during vigorous sports. In contrast with severe head traumas that might cause irreversible neuronal injuries, repeated mild head injuries rarely induce destructive brain injuries. The effect of this trauma is usually transient; however, it has been reported that prolonged and repeated concussions cause permanent cognitive impairment.8)10)13)
We treated a young football player who presented with acute subdural hematoma, cerebral edema, and seizure due to a ruptured pseudoaneurysm of middle cerebral artery (MCA). Through surgical findings and literature review, we were convinced that the pseudoaneurysm with dural calcification and adhesion on underlying brain may have been formed by repeated concussions.
CASE REPORT
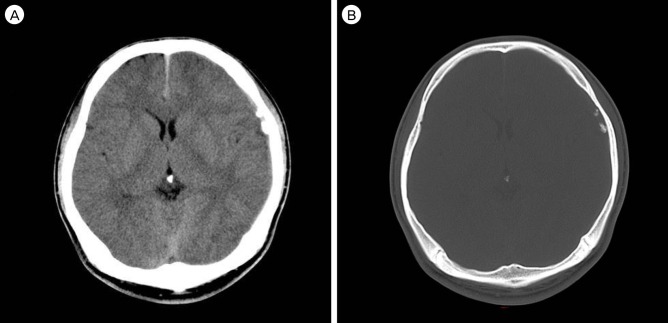
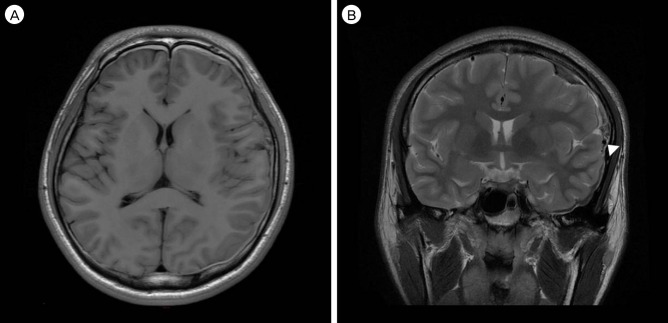
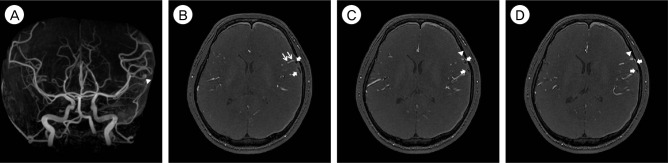
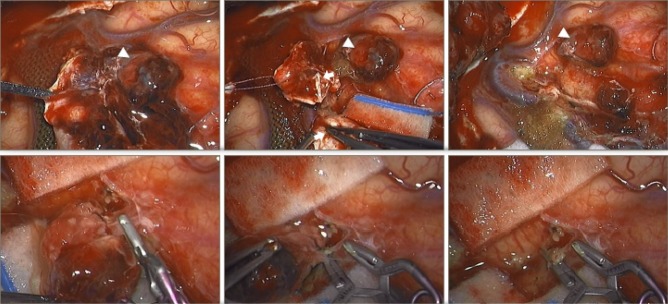
An 18-year-old American college football player presented with a vague headache since he was tackled during exercise several weeks ago. Brain computed tomography (CT) was performed at a local hospital a few days before visiting our hospital because the headache worsened and was not relieved through medication. Initial brain CT revealed a small amount of subdural hematoma on the left cerebral convexity (Fig. 1). Few calcified nodules were noted at the left frontotemporal cortex. However, it was initially considered a simple traumatic hemorrhage and was managed by conservative means. Several days later, the headache aggravated and the patient experienced an episode of generalized partial seizure. On the magnetic resonance imaging (MRI) performed immediately after the seizure, the size of acute hematoma and cerebral edema was markedly increased, and a small enhancing mass was observed at the left cerebral convexity (Fig. 2). Magnetic resonance angiography (MRA) revealed a 4 mm sized aneurysmal dilatation of the cortical branch of the MCA, which supplies the superior temporal region (Fig. 3). Emergency craniotomy was performed to eliminate the aneurysm and lower the elevated intracranial pressure by removing the hematoma. A large craniotomy was done, and the subdural hematoma was removed by repeated gentle irrigation and suction after small dural incision. While further opening of the dura, we were encountered by several irregularly shaped, hard subdural nodules which were tightly adhered to the dura and the underlying brain (Fig. 4). Upon careful dissection, these nodules were noted to be buried in the sulcus while being severely adhered to the brain cortex and the cortical arteries. Between the nodules was an organizing hematoma and upon careful removal, a pseudoaneurysm of the cortical MCA branch was exposed. The involved MCA branch was carefully dissected and was trapped by clips at the proximal and distal portion of the severely injured and adherent segment, along with the pseudoaneurysm. The aneurysm and the calcified nodules were then excised. The ischemic injury was minimized because the collateral flow retrogradely supplied the distal part of the occluded artery. The patient recovered without sequelae and was discharged after a short while.
DISCUSSION
Traumatic brain injury is common among football players. Approximately 300,000 sport-related concussions occur annually in the United States, and the likelihood of serious sequelae might increase with repeated head injury.7)19) Many studies about repeated head injuries have been published, and subdural hematoma is known as the most common cause of brain injury-related fatality in sport-related injuries.5)6)17) Subdural hematoma occurs due to severe head trauma such as skull fracture, but not by minor head trauma. Brain injury-related fatalities are dramatically reduced by wearing protective helmets that prevent severe head trauma.6) Most of the reports about repeated mild brain trauma focus on neurodegeneration.2)3)4) Our case differed from the reported cases in the context that repeated brain injury may have formed calcification of the dura over a long period of time, which in turn may have caused mechanical irritation and injury of the MCA branch, resulting in pseudoaneurysm formation and rupture.
Pseudoaneurysm formed at the cortical MCA in minor blunt head trauma was very unusual because the location of pseudoaneurysms reflects the mechanism of injury. For example, basal skull fracture might cause pseudoaneurysm at the vertebrobasilar system.11)14)15)21) Arterial contusion by the anterior clinoid process causes supraclinoid internal cerebral artery pseudoaneurysms.14)15) Distal anterior cerebral arteries might be injured by the proximal falcine edge.16) Cortical artery aneurysms commonly form because of an overlying skull fracture.21)
However, these general injury mechanisms could not explain our case. Hence, we focused on the dural calcification in the initial brain CT.
Calcification of the intracranial dural meninges is rare; however, it may occur due to degeneration, irritation, inflammation, hemorrhage, or trauma.1)12)20)22) For example, calcifications might develop in chronic subdural hematomas due to trauma and inflammation and the degree of calcification extends from thin calcified inner membranes to dense calcification, including ossification of the hematoma.1)12) The physiology of dural calcification has not been fully understood; however, it might be due to calcium and, sometimes, iron deposition in the blood vessels of different structures of the brain.1)9)
Applying this hypothesis to our case, we conjectured that the repetitive concussion and inflammation might be the cause of dural calcification and its adherence to the brain. The cortical MCA pseudoaneurysm may have arisen from mechanical irritation of the arterial wall by the adherent dural calcification, resulting in subsequent arterial wall shear and tear. The adhesion of calcified dura mater on the injured brain was confirmed in the operation field.
The most common clinical presentation of traumatic pseudoaneurysm is delayed intracranial hemorrhage with subsequent neurological deterioration; however, it can be prevented by early diagnosis.15)18) Hence, traumatic pseudoaneurysm must be taken into consideration even in mild traumatic brain injury, along with all other entities. Among patients with repeated mild head trauma, if acute subdural hematoma is seen in the brain CT, traumatic pseudoaneurysm must be suspected and angiographic evaluation, either direct or indirect, should be attempted immediately.
Traumatic pseudoaneurysms rarely regress spontaneously and have a high incidence of rupture and mortality.14)21) Hence, treatment should be performed immediately if traumatic pseudoaneurysm is diagnosed. Surgical treatment including clipping, excision of the aneurysm, coiling or wrapping, should be considered.
In our case, unusual calcification found in the initial CT was the clue of diagnosis. Prompt MRA was performed under the suspicion of pseudoaneurysm due to this calcific nodule and the patient's history of repeated head injury. After prompt work-up and successful surgical management, the patient was treated before fatal rebleeding and discharged home without any sequelae.
CONCLUSION
We report an unusual case where a traumatic pseudoaneurysm was the cause of an acute SDH after repeated mild head injury. We speculate the repeated injury to the head may have resulted in chronic formation of dural calcification, which in turn may have resulted in mechanical injury of the cortical MCA branch. When calcified nodules are seen in the initial CT scan of such patients, pseudoaneurysms must be taken into consideration as the underlying cause.
 XML Download
XML Download