

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With the improvement in catheter technology, the large bore catheter can be advanced into distal tortuous vessels for manual aspiration thrombectomy (MAT). Using this type of catheter has shown improvements in recanalization rates and favorable clinical outcomes as stent retriever thrombectomy.12)17)18) Although contrast leakage and subarachnoid hemorrhage (SAH) have been reported during and after MAT, pseudoaneurysm formation due to vessel wall injury has not been.2)6)7)8)9)10)11)12)13)14)15)17)18) We therefore report on a case of significant contrast leakage during MAT in which we found pseudoaneurysm formation at follow-up angiogram that was treated by detachable coil embolization. We also discuss the pathogenetic and therapeutic considerations of our case.
Go to : 
CASE REPORT
A 60-year-old woman arrived at our emergency room with complaints of dysarthria and left-sided weakness, which had abruptly started 1 hour and 40 minutes previously. Magnetic resonance imaging and magnetic resonance angiography (MRA) showed right proximal middle cerebral artery (M1) occlusion with partial infarction in the middle cerebral artery (MCA) region. And perfusion weighted image confirmed perfusion weighted image-diffusion weighted image mismatch. We decided to perform a thrombectomy with the patient in a conscious, sedated state, without intravenous t-PA(tissue plasminogen activator), because we could perform a thrombectomy immediately. On initial angiogram, right mid M1 occlusion was confirmed, and MAT using an aspiration catheter (Penumbra 5MAX, Penumbra Inc., Alameda, CA, USA) and 50 mL syringe was performed four times until M1 was recanalized (Fig. 1A, B, C). Before each suction thrombectomy, the Penumbra suction catheter was carefully navigated to the occlusion point while suction catheter loaded with a Prowler Select Plus (Codman, Raynham, MA, USA) microcatheter and Synchro (Stryker; Kalamazoo, MI, USA) microwire coaxially. However, one of the distal branches (M2) was occluded. We attempted another MAT using an aspiration catheter with a smaller inner diameter (Penumbra 4MAX) (Fig. 1D). On the follow-up angiogram after the fifth MAT, we noticed recanalized M2 and significant extravasation of contrast at the distal M1 segment (Fig. 2A). We stopped the procedure because further runs of angiogram show diffuse vasospasm and no more contrast leakage. On postoperative computed tomography (CT) of the brain, diffuse SAH on the right Sylvian fissure and multiple sulci were noted with accompanying ventriculomegaly (Fig. 2B). The patient was conscious, albeit drowsy, and we drained her cerebrospinal fluid via a lumbar drain. She showed improvement of consciousness on the next day, and we continued conservative treatment. On the follow-up CT, SAH along the Sylvian fissure persisted until postoperative day (POD) 12, when the patient showed deterioration of consciousness. On the angiogram, vasospasm was noted on right M2 segments, and chemical angioplasty using Nicardipine (Perdipine, Astellas, Shizuoka, Japan) was performed daily for three days (Fig. 2C). On the angiogram taken on POD 15, a tiny pseudoaneurysm (Fig. 2D, E) was found at the origin of the small temporal branch of the right M1, and embolization using detachable platinum coils was successfully performed under general anesthesia (Fig. 3A, B). The location of the pseudoaneurysm was distal to the original occlusion site and near the segment where the contrast leakage started. The patient showed improvement of consciousness later and was discharged rehabilitation with only mild weakness while making grasping motions with her left hand. On the follow-up angiogram obtained on post-embolization day 17, contrast filling in the pseudoaneurysm was not observed (Fig. 3C). An MRA obtained on post-embolization day 125 showed no evidence of a remnant sac (Fig. 3D).
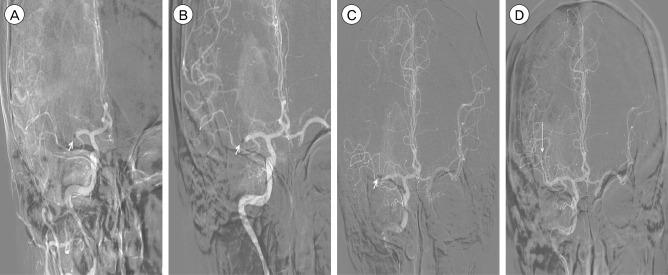 | Fig. 1Digital subtraction angiography (DSA) roadmap images during thrombectomy. (A) Roadmap shows right middle cerebral artery, mid M1 segment occlusion, and the suction catheter tip (Penumbra 5MAX, Penumbra Inc., Alameda, CA, USA) for the first manual aspiration thrombectomy (MAT) (arrow). (B) For the second MAT, the roadmap shows more distal M1 occlusion than seen in the angiogram performed after the first MAT and the suction catheter tip (arrow). (C) Roadmap shows right distal M1 segment occlusion after the third MAT and suction catheter tip for the fourth MAT (arrow). (D) Roadmap shows one M2 branch occlusion by migrated thrombus and suction catheter (Penumbra 4MAX) tip for the fifth MAT (arrow).
|
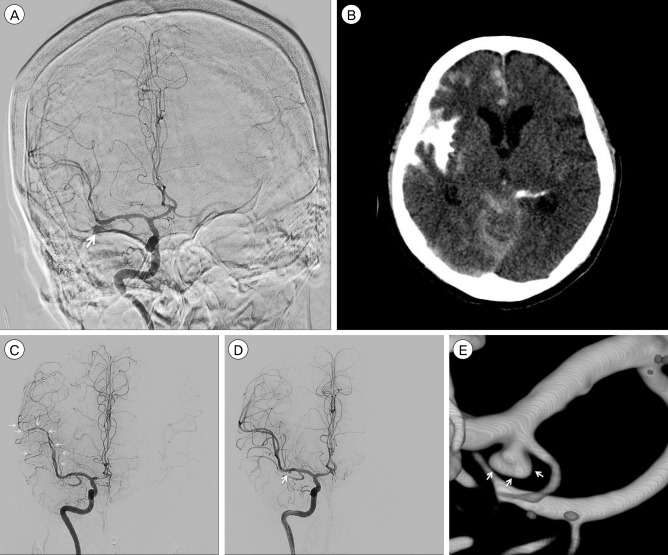 | Fig. 2Digital subtraction angiography (DSA) and three-dimensional reconstruction images, computed tomography (CT) after thrombectomy. (A) DSA shows contrast leakage (arrow) at distal M1 near the fourth MAT point. (B) CT shows diffuse SAH on the right Sylvian fissure and multiple sulci accompanying ventriculomegaly (C) DSA performed on postoperative day (POD) 12 shows multiple vasospasms at M2 and M3 segments (arrows) and no evidence of an aneurysm sac. (D) DSA performed on POD 15 shows an aneurysm sac near the extravasation site (arrow). (E) Three-dimensional reconstruction image of pseudoaneurysm at the origin site of small temporal branch of the right M1 segment (arrow).
|
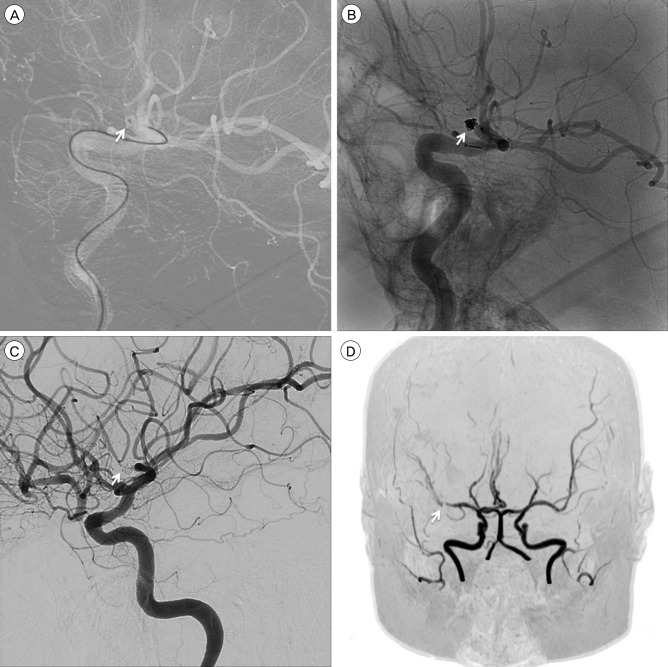 | Fig. 3Angiograms obtained during embolization and the follow-up period. (A) Digital subtraction angiography (DSA) roadmap image shows a single microcatheter selected into the pseudoaneurysm sac (arrow). (B) Non-subtracted angiography shows no contrast filling in the pseudoaneurysm after detachable coil embolization (arrow). (C) DSA performed on postoperative (POD) day 17 shows complete occlusion of the pseudoaneurysm (arrow). (D) Magnetic resonance angiography performed on POD 125 shows no evidence of a remnant sac (arrow).
|
Go to :
DISCUSSION
Aneurysm is classified into true aneurysm and pseudoaneurysm histologically. True aneurysm refers to an aneurysm that is formed due to incomplete injury to the vascular wall with existing adventitia. In contrast, pseudoaneurysm forms a false lumen with completely disrupted vascular wall. In our case, hematoma formed around vessel injury site, so no abnormal finding observed around vessel injury site in follow-up digital subtraction angiography. As time goes by hematoma resolved, false lumen formed around vessel injury site. We observed pseudoaneurysm in follow up angiogram due to contrast filling in false lumen.
With the improvement of endovascular techniques and devices, the demand for endovascular recanalization for major intracranial artery occlusion is increasing. Because of the improvement in catheter engineering, it is possible to navigate the relatively large bore catheter into the tortuous distal cerebral vessels. In reports comparing MAT using this kind of catheter between stent retriever, clinical outcome, complication, recanalization rate did not differ significantly.15)17) So as thrombectomy using stent retriever, MAT became one of the two current standard of thrombectomy for patients with acute cerebral artery occlusion.
During and after MAT in patients with acute occlusion, the rates of contrast leakage and SAH have been reported to be between 0% and 31%.2)6)7)8)9)10)11)12)13)14)15)17)18) Intra-procedural vessel perforation occurs in 1.1-2.6% of patients and vessel dissection in 4.4-4.5%.2)7)8)10) Distal catheter's outer diameters for stent retriever thrombectomy is 2.3-2.7F, while distal catheter's outer diameters for MAT is 3.8-5F. Considering that MAT is carried out with catheters that have relatively larger diameters than catheter diameters for stent retriever thrombectomy, the possibility of vessel injury exists and is higher. Furthermore, it is inevitable for the vessel wall distal to the occlusion to become vulnerable to trauma by the catheter tip because of ischemic injury as the duration of occlusion increases. Hence, it is recommended to limit the number of passes of the Solitaire stent retriever (ev3, Irvine, CA, USA) to three for one vessel.1) There is no reports about such limitation, however, for the Penumbra suction catheter. Therefore, although the frequency is very low, operators who perform MAT should remember that vessel injury and even formation of pseudoaneurysm could occur during procedures and pass suction catether in patient's cerebral artery as little as possible. Considering that the pseudoaneurysm was visualized on angiogram on POD 15 in our case, frequent follow-up with imaging studies is mandatory, especially for a few weeks after vessel injury.
For blocking the inflow of blood to the pseudoaneurysm from the parent artery, neck clipping and coil embolization can be considered. Although clipping has the advantage of more complete vessel wall repair and concomitant hematoma removal,16) it could possibly lead to premature rupture during the dissection step. Clipping is also technically difficult, particularly in patients with increased intracranial pressure.3)5) With recent developments in instruments and techniques, good results have been reported for endovascular coil embolization of pseudoaneurysms.3)4) Similar to the patient in our case, patients with severe edema and vasospasm can be good candidates for embolization. The short-term follow-up results of this case reconfirm those of previous reports and long-term follow-up is mandatory.
Go to :
CONCLUSION
We experienced significant contrast leakage during repetitive suction thrombectomy for a patient with acute MCA occlusion that later became a pseudoaneurysm. Surgeons who perform suction thrombectomy should be keep in mind catheter diameters for suction thrombectomy and aware of possible vessel injury that results in the formation of pseudoaneurysm during and after procedures, particularly at the branching site or tortuous segments.
Go to :
 XML Download
XML Download