

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The middle meningeal artery normally arises from the proximal maxillary artery and enters the middle cranial fossa through the foramen spinosum to supply the dura and the calvarium.2)3) It can serve as an endovascular route for devascularization of a variety of dural-based neoplastic processes and even cure in the case of dural arteriovenous fistulae. Anatomical variants of the origin of the middle meningeal artery (MMA), arising from the ophthalmic artery, internal carotid artery, and persistent stapedial artery have been reported in the literature.2)3)6) We report on a rare aberrant MMA originating from the basilar artery (BA), with discussion of its anatomic and clinical significance.
CASE REPORT
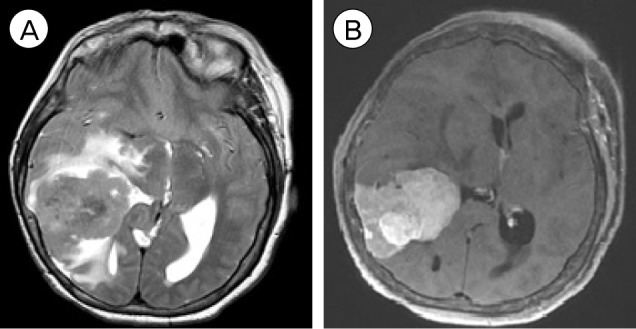
A 54-year-old right handed white female presented to the emergency department complaining of frequent headaches over a 6-month period. On examination, she had a left-sided pronator drift, mild spasticity of the left lower extremity, and hypoesthesia of the left side of her body. She underwent brain magnetic resonance imaging, which showed a 3 × 4 cm sized right parietal dural-based soft tissue mass with radiographic characteristics consistent with meningioma. A considerable amount of surrounding vasogenic edema was observed with approximately 6 mm of midline shift (Fig. 1).
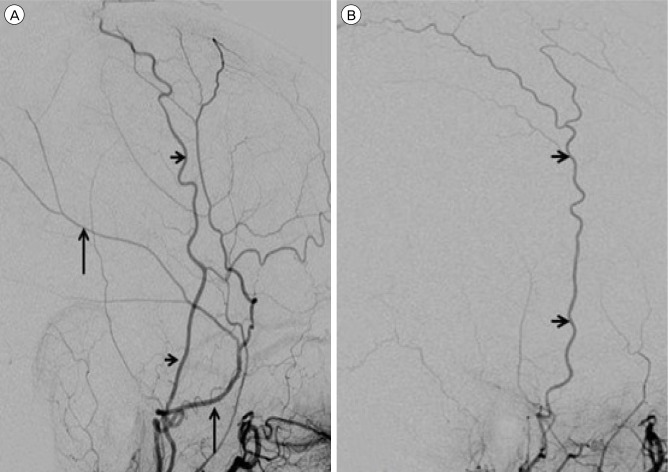
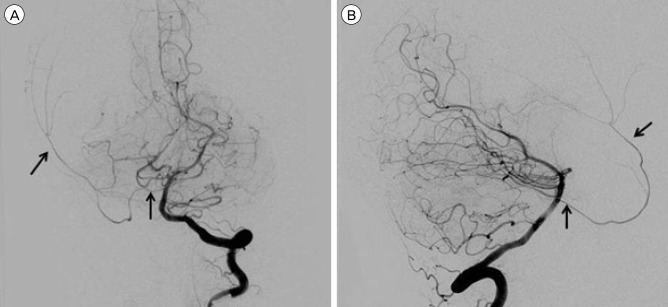
Six-vessel conventional cerebral angiography was performed for possible pre-operative embolization of the tumor. Injection of the left external carotid artery (ECA) showed normal anatomy, origins and configuration of the left internal maxillary, MMA and accessory MMA without contributing feeders to the tumor (Fig. 2A). Injection of the right ECA showed that the right internal maxillary artery had a small accessory MMA but no MMA or tumor blush (Fig. 2B). Injection of the left vertebral artery showed a dominant left vertebral system with the MMA arising from the upper basilar trunk (Fig. 3). It provided some blood supply to the tumor; however, when weighed against its benefit, the risk of embolization via this route was deemed unsuitable.
DISCUSSION
The diverse variants of anatomy of the MMA are due to its complex embryological development. The MMA develops from the stapedial artery, which originates from the dorsal stem of the second arch artery.3) It passes through the ring of the stapes to anastomose with the cranial end of the ventral pharyngeal artery. The stapedial artery contains three branches, mandibular, maxillary, and supraorbital, which distribute along the divisions of the trigeminal nerve. The external carotid artery arises from the base of the third arch and assimilates the stem of the ventral pharyngeal artery. Its internal maxillary branch communicates with the common trunk of the maxillary and mandibular branches of the stapedial artery and incorporates these vessels. The proximal part of the common stem forms the root of the middle meningeal artery. The distal part of the MMA is derived from the proximal part of the supraorbital artery, which is a branch of the ophthalmic artery. At this stage, the proximal part of the stapedial artery regresses and its remnants form the tympanic branches of the MMA.3) After this complex developmental stage, the MMA passes between the sphenomandibular ligament, the lateral pterygoid muscle, and two roots of the auriculotemporal nerve and enters the floor of the middle cranial fossa through the foramen spinosum. It then passes laterally through a crest in the greater wing of the sphenoid bone, subsequently dividing into frontal and parietal branches.2) Upon entering the cranium, the middle meningeal artery gives off several small branches supplying the trigeminal ganglion and the dura, as well as giving rise to superficial petrosal and orbital branches.3)
Various reports of anomalous origins of the MMA have been published.2) The ophthalmic origin of the MMA is a frequently encountered anomaly,6) which may arise partially or completely from the ophthalmic artery. In addition, the MMA can originate from the extradural or the intra cavernous portions of the internal carotid artery.6) Rarely, it may arise as a branch of the persistent stapedial artery, and even less frequently from the ascending pharyngeal artery.6)
Our case represents the ninth reported patient in the literature with an MMA arising from the basilar artery.1)4)5)7)8)9) In review of the reported cases, these findings have been made in infants, children, and adults without a clear sex predilection. In five cases, it arose from a lateral pontine branch of the basilar artery; in the remaining cases it arose from the basilar artery, most often between the superior cerebellar artery and anterior inferior cerebellar artery.1)4)5)7)8)9) In one case, both MMAs arose directly from the basilar artery.4)
The first case reported by Altman was an abnormal vessel in a 7-month fetus post mortem called the "acoustic-facial artery" arising from the basilar artery between the AICA and PICA, passing through the right internal auditory canal and continuing as the MMA.1) Seeger and Hemmer published three cases of the MMA originating from the hypertrophied pontine branches of the basilar artery.7) Two different explanations for this abnormal origin were offered: 1) anastomosis between the lateral pontine branch of the basilar artery and trigeminal branches of the MMA or 2) anastomosis between the primitive trigeminal and the MMA. Wagaet al. reported another case of the MMA originating from the BA, postulating that this anastomosis can form between the trigeminal artery of the lateral pontine branch and the MMA.9) A bilateral case of MMAs originating from the basilar artery was noted by Katz et al. during treatment of a ruptured ACOM aneurysm.4) A more recent study by Shah and Hurst described a left MMA originating from the lateral pontine branch of the basilar artery.8) The authors hypothesized that the embryological mechanism of this anomaly is related to the persistent anastomosis between the intracranial components of the stapedial artery and lateral pontine artery in the region of trigeminal ganglion.
Kumar and Mischra reported a case of MMA originating directly from the left side of the basilar artery trunk.5) The authors explained this anomalous origin as a persistent perineural arterial anastomosis in the trigeminal ganglion region, formed by branches of the developing stapedial and basilar arteries. This reported case is very similar to our current patient, in whom the right MMA originated directly from the basilar trunk.
The posterior circulation origin of an MMA supplying an endovascular target such as an arteriovenous shunt or dural-based neoplasm has significant clinical implications as nuances of successful catheterization and, more importantly, reflux of embolization materials can have significant consequences. In our case, considering these possible risks, we decided against embolization.
CONCLUSION
The aberrant origin of the MMA from the BA is very rare; however, this variant is of crucial importance in planning any neuroendovascular procedure. Knowledge of the abnormal anatomy and its potential collateral connections is essential to prevention of serious complications such as possible refluxing of the embolization agent during the procedure.
 XML Download
XML Download