

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Giant intracranial aneurysms are associated with a dismal natural history due to their high propensity for rupture.20) Traditional surgical treatment and endovascular approaches are associated with high complication rates.2)9)15) In addition, endovascular coiling of giant aneurysms without concomitant stenting is associated with relatively high rates of recurrence.13) The recent addition of flow-diverting stents (FDS) to the endovascular armamentarium has resulted in drastic improvement of the ability to administer safe and effective treatment of giant aneurysms.1)14) Successful deployment of a FDS across an aneurysm neck is predicated upon microcatheter access to the distal segment of the parent artery past the aneurysm neck. Giant aneurysms have strong inflow jets, which direct microcatheters into the aneurysm sac, where redundant catheter loops are deposited prior to accessing the distal parent artery. Inability to create a direct path across the neck of a giant aneurysm may preclude use of an endovascular approach. Anchoring techniques to assist in gaining direct access of a microcatheter distal to the aneurysm neck without traversing the aneurysm sac have been previously described.3)10)11)19) We report on the first case of a balloon anchor technique used to navigate across a giant aneurysm in order to facilitate treatment with a FDS.
CASE REPORT
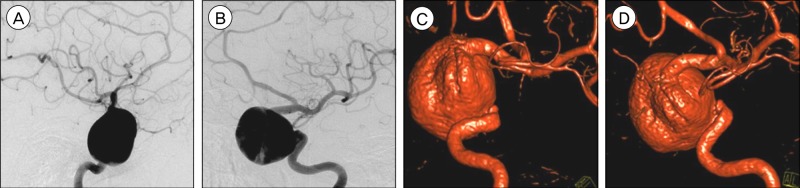
A 59-year-old female presented with headache and fatigue secondary to profound hypopituitarism. Initial noninvasive neuroimaging and subsequent catheter cerebral angiography identified a giant (2.9 cm in maximal diameter) supraclinoid internal carotid artery (ICA) aneurysm arising from the branch point of the superior hypophyseal artery (SHA) extending into the sella turcica (Fig. 1). Given the size and location of the aneurysm, the decision was made to treat the patient using an endovascular approach using the Pipeline Embolization Device (PED, ev3, Plymouth, MN, USA). The patient was premedicated with aspirin 325 mg daily and plavix 300 mg single loading dose followed by 75 mg daily for three days prior to undergoing the stent procedure. Results of the patient's aspirin and plavix assays showed therapeutic levels of platelet inhibition at 350 aspirin reaction units (ARU, therapeutic level < 551 ARU) and 177 P2Y12 reaction units (PRU, therapeutic level < 208 PRU), respectively.
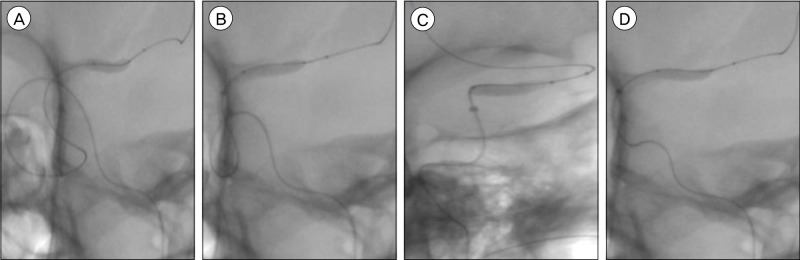
A ReFlex 058 guide catheter (Reverse Medical, Irvine, CA, USA) was navigated into the left ICA through a Flexor Shuttle 087 guiding sheath (Cook Medical, Bloomington, IN, USA), so that control angiograms could be performed during the stent procedure. Initially, a Marksman microcatheter (ev3) was advanced past the aneurysm into the left middle cerebral artery (MCA) trunk. The PED was advanced through the Marksman microcatheter, however, catheter herniation into the aneurysm, caused by the course of blood flow through the giant aneurysm sac, precluded effective stent placement and delivery of the stent past the aneurysm neck. Therefore, the Marksman microcatheter and PED were removed and the decision was made to use a balloon anchor technique to improve endovascular access across the aneurysm neck (Fig. 2). Next, a Scepter C balloon (MicroVention, Tustin, CA, USA), placed within a DAC 044 catheter (Concentric Medical, Mountain View, CA, USA), was advanced over a Transend 014 microguidewire (Boston Scientific, Natick, MA, USA) to the left SHA aneurysm.
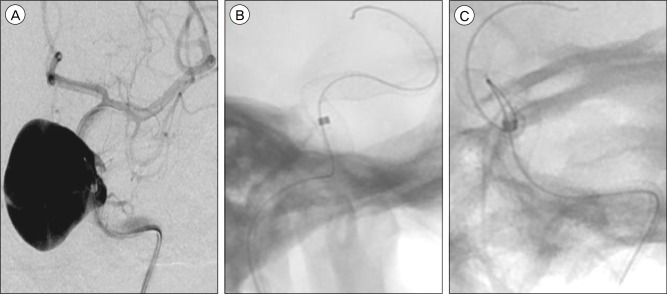
Under continuous fluoroscopic guidance, the Scepter C balloon was advanced into the left MCA and inflated. With the balloon serving as an anchor, the DAC 044 catheter was advanced through the aneurysm into the supraclinoid ICA. There was a significant amount of catheter redundancy within the aneurysm sac. By slowly pulling down the DAC 044 catheter, the length of redundant catheter within the aneurysm sac showed a gradual decrease until the catheter was only traversing the aneurysm neck. The Scepter C balloon was then deflated and removed from the patient. Next, an Excelsior XT-27 microcatheter (Stryker, Kalamazoo, MI, USA) was advanced through the DAC 044 into the supraclinoid ICA distal to the aneurysm neck. A 5.0×30 mm PED was then advanced through the XT-27 microcatheter and deployed across the aneurysm neck in a standard fashion. Post-PED control angiogram through the ReFlex 058 guide catheter showed two narrowed sections along the stent (Fig. 3). A J-shaped microguidewire was navigated through the PED construct over which a TREK 3×12 coronary balloon (Abbott Vascular, Abbott Park, IL, USA) was advanced in order to perform angioplasty on the stenotic segments of the PED. Final control angiography showed increased flow stasis within the aneurysm, compared to pre-treatment angiography, without evidence of intraprocedural complications (Fig. 3). The patient's postprocedural course was uneventful. She was discharged home two days after undergoing the endovascular procedure without neurological deficits. Follow-up computed tomography angiography at six months and diagnostic catheter angiography at one year showed a significant reduction in aneurysm size. The patient will continue to be monitored with serial angiography for progressive aneurysm thrombosis.
DISCUSSION
Although endovascular embolization has not been rigorously compared to surgical clipping for treatment of unruptured aneurysms in a prospective, randomized trial, there has nonetheless been a significant shift in the management of unruptured aneurysms away from surgery toward endovascular techniques.17)18) The most recent expansion of the endovascular armamentarium has been the development of FDSs.12) Although many of the initial lesions with FDSs were giant aneurysms located on the ICA proximal to the posterior communicating artery, recent studies have expanded the role of FDSs for small aneurysms, including blister subtypes, anterior circulation aneurysms located distal to the supraclinoid ICA, posterior circulation aneurysms, and ruptured aneurysms.4)5)7)16) However, prudent use of these novel devices is paramount to optimizing endovascular outcomes for aneurysm patients. Since the collective experience with FDSs is relatively lower than with coils, the management and technical nuances of FDSs are still being defined.6)8)
Flow diversion using endovascular stents, such as the PED and SILK stent (BALT Extrusion, Montmorency, France), provide a powerful therapeutic approach as they can lead to aneurysm obliteration without compromise of the parent vessel. Proximal occlusion of the parent artery is not always feasible in cases of inadequate collateral arterial supply when hypoperfusion of the supplied territory may result in ischemic neurological deficit. Both low porosity FDSs and high porosity traditional stents require endovascular navigation of a microcatheter across the aneurysm neck. In cases of non-thrombosed giant aneurysms, which have particularly high flow inlet arterial jets, such as the one in the case presented, the preferential path of a microcatheter is into the aneurysm sac rather than across the neck, which prohibits stent deployment. Alternative treatment options not requiring endovascular access to the distal parent artery are (1) surgical clipping with clip reconstruction of the parent artery, (2) surgical parent artery occlusion with or without distal extracranial-intracranial bypass, (3) endovascular parent artery occlusion with a balloon or coils, (4) aneurysm embolization alone with coils or Onyx (ethylene vinyl alcohol copolymer, ev3), and (5) balloon-assisted embolization.
Stent-assisted coil embolization using traditional, high porosity intracranial stents is another potential treatment strategy; however, this approach also required access to the distal parent artery. Vascular tortuosity, which is often associated with giant aneurysms, requires significant catheter support systems to enable successful navigation of FDSs across the aneurysm neck. This is also required in order to reduce the probability of stent herniation within giant aneurysms. Use of alternative microwires and microcatheters with increased stiffness may facilitate passage across the aneurysm neck without entrance into the sac and avert usage of a balloon anchor technique. However, stiffer endovascular support wires increase the risk of arterial dissection and aneurysm rupture. Therefore, use of the balloon anchor technique enables passage of a relatively soft microcatheter directly across the aneurysm neck in order to enable stent-assisted endovascular reconstruction of the diseased parent artery.3)19) Cekirge et al. first described the balloon anchor technique for the treatment of two giant ICA aneurysms, one with combined balloon- and stent-assisted coil and Onyx embolization and the other with covered stent occlusion.3) Subsequently, Snyder et al. reported the use of a balloon anchor technique for stent-assisted coil embolization of a giant ICA aneurysm.19) Under a similar premise, Fargen et al. described a stent anchor technique for obtaining distal access across large aneurysms.11) Most recently, Edwards et al. described a 'sea anchor' technique, utilizing a long segment of partially deployed coil to increase the drag of the distal microcatheter and effectively act as a hemodynamic anchor.10) Our unique case represents the first use of a balloon anchor technique to assist in deployment of a FDS for the treatment of a giant supraclinoid ICA aneurysm.
CONCLUSION
FDSs, such as the PED, have revolutionized endovascular approaches for treatment of complex intracranial aneurysms for which traditional endovascular and surgical techniques are associated with significant treatment-related complication rates. Direct microcatheter access across the neck of an aneurysm is a critical step prior to deployment of a FDS. Due to the powerful inflow jets and vascular morphology associated with some giant aneurysms, microcatheters are directed into the aneurysm sac where one or more redundant loops are deposited prior to accessing the distal parent artery. A balloon anchor technique may be used for safe achievement of a direct and effective microcatheter position across the neck of a giant aneurysm to enable treatment of these lesions using FDSs.
 XML Download
XML Download