

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anterior communicating artery (ACoA) is the most common site for intracranial aneurysms as revealed by landmark clinical studies.4) Despite the high prevalence of ACoA aneurysms, surgical clipping of ACoA aneurysm can still be challenge to even experienced neurosurgeons because of variable anatomy of the ACoA complex and its surrounding structures. The selection of the best surgical approach should include minimum brain retraction, minimum unnecessary operative manipulation, familiarity of surgical approach for operator, and easy access to the aneurysm, which depends on location, direction and size. The selection of surgical approach for high-positioned ACoA aneurysm can be even more difficult because surgical obliteration of high-positioned ACoA aneurysm requires higher technical skill and the use of adjunct procedures, such as, extended craniotomy, resection of gyrus rectus, and revascularization techniques. In 1953, Norlen and Barnum first described a transfrontal approach for ACoA aneurysm with partial resection of frontal lobe.5) Kempe and VanderArk published a modified transfrontal approach with limited rectus gyrus resection.3) Nevertheless, a conventional pterional approach with resection of rectus gyrus is still used for the surgical obliteration of ACoA aneurysm. In our institution, we modified procedures from the conventional pterional approach. We dissect the olfactory tract and detach from frontal lobe. In this study, the purpose is to evaluate surgical outcome of our pterional-subolfactory approach for the high positioned ACoA aneurysm through comparison with conventional pterional approaches.
MATERIALS AND METHODS
Between February 2005 and December 2012, 463 ACoA aneurysms were surgically treated in our institution. Among them, 48 high positioned anterior communicating aneurysms were treated with pterional-subolfactory or conventional pterional approaches. The pterional-subolfactory approach includes sharp dissection and detachment of olfactory tract to free from brain parenchyme and resection of the gyrus rectus immediately medial and inferior to the olfactory tract. Thirty-four of the 48 cases were treated with pterional-subolfactory approach and 14 were treated conventionally. High positioned anterior communicating artery aneurysms were defined as aneurysms located higher than 10 mm above the anterior clinoid process.
Preoperative radiologic assessment
Preoperative computed tomography angiography (CTA) or digital subtraction angiography (DSA) was performed to characterize ACoA aneurysms for all 48 patients. Simple skull anterior-posterior and lateral were checked to identify frontal sinus. The height of aneurysm was measured as height from anterior clinoid process to neck of aneurysm on maximum intensive projection sagittal view of CTA or DSA. Preoperative subarachnoid hemorrhage and intracranial hemorrhage were checked on CT.
Surgical technique
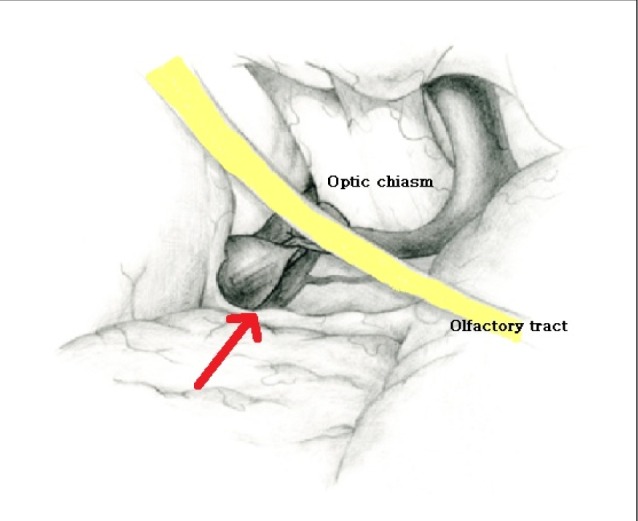
The operation was performed with the patient in a supine position. The head was rotated about 15 degrees to the opposite side of aneurysm and extended 10 to 20 degrees toward the floor, then was fixed in a sugita 4-pin head frame. We performed the standard pterional approach by drilling the skull base. We dissected the sylvian fissure to identify optic nerve, internal carotid artery (ICA), ipsilateral and contralateral A1 segment. After identifying both A1 segments, we deduced the location of aneurysm. In conventional pterional approach, we usually elevated the frontal lobe with a retractor over the olfactory tract. In contrast, the pterional-subolfactory approach sharply dissect the olfactory tract, detaching it from the frontal lobe to free from the brain parenchyma (Fig. 1). We then cauterized the rectus gyrus, immediately medial and inferior of olfactory tract. Using the suction and the bipolar cautery, we resected the rectus gyrus until the medial side pia arachnoid of the gyrus rectus was recognized over the aneurysm and the ipsilateral A1 and A2 segments. After the proper recognition of high positioned aneurysm, we safely obliterated the aneurysm while it was directly visualized.
Outcome assessment
The clinical and radiologic outcomes were evaluated retrospectively according to the following methods. All patients' charts, medical records and radiologic examinations were reviewed. Postoperative clinical outcomes were measured by means of Glasgow outcome scale (GOS). All the postoperative images were analyzed by neuro-specialized radiologist for postoperative complications, such as hemorrhage, cerebral contusion, remnant aneurysm and venous infarction. Postoperative complications such as postoperative infarction, perforating artery injury, infection and cerebrospinal fluid leakage were checked.
RESULTS
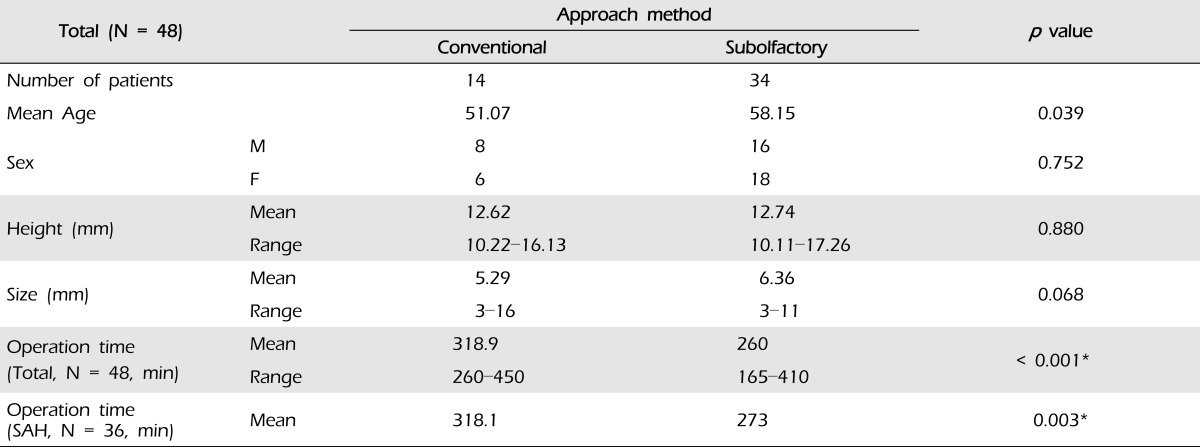
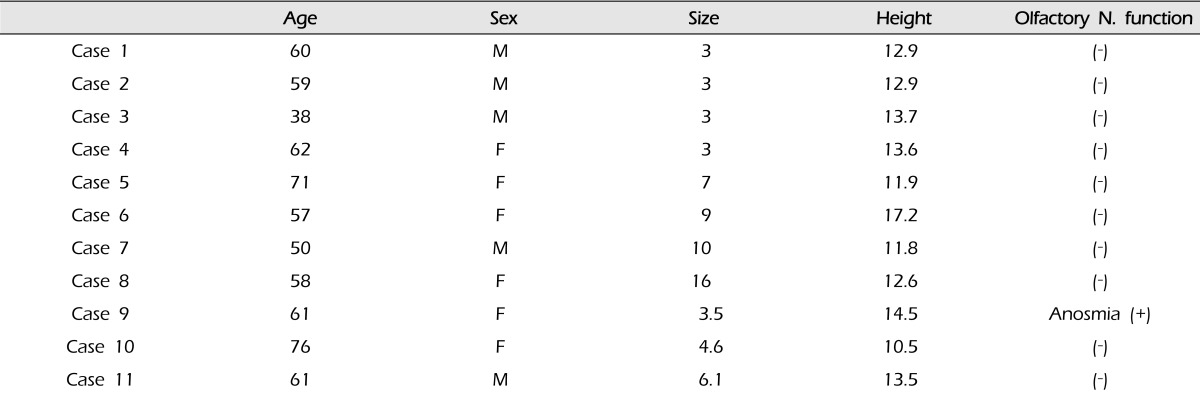
For the 34 cases treated with pterional-subolfactory approach, the mean location of ACoA aneurysm was 12.62 mm (range from 10.22 to 16.13 mm) from the anterior clinoid process. For the 14 cases treated with conventional approaches, the mean location of ACoA aneurysm was 12.74 mm (range from 10.11 to 17.26 mm). Sizes of aneurysms treated with subolfactory approach were varied from 3 mm in diameter to 16 mm (average 5.52 mm in diameter). The average diameter of conventionally treated aneurysms was 6.36 mm. The operation duration for conventional pterional and pterional-subolfactory approaches were measured, and conventional pterional approach took 58 minutes more than the pterional-subolfactory approach (p = 0.001). Patient characteristics are summarized in Table 1.
Clinical and surgical complication
Complications occurred in 2 cases of the conventional pterional approach group, and 1 case in pterional-subolfactory group. Postoperative cerebral infarction developed in 2 cases with the conventional pterional approach, but not in the pterional-subolfactory approach group (p = 0.026, Table 2). In 1 case, long hours of temporary clip usage resulted in postoperative cerebral infarction on right frontal lobe and permanent neurologic deficit. In the other case, postoperative cerebral infarction due to perforate artery injury developed; however, patient was discharged with no remnant neurologic deficit. One case of postoperative intracranial hemorrhage occurred in the pterional-subolfactory approach group, none in the conventional pterional approach group, but the difference was not statistically significant (p = 0.51, Table 2). Cerebro-spinal fluid leakage and postoperative wound infection did not occur in either group.
Radiologic results for remnant aneurysm
Postoperative CTA or DSA was performed to evaluate remnant aneurysm for all 48 patients. Surgical clipping was successfully performed in all patients except for 1 case with the conventional pterional approach. In that case, postoperative DSA revealed severe remnant with flow in aneurysm. We then, underwent revision operation for repositioning of clip. After reposition of clip, DSA was performed, and revealed complete obliteration of aneurysm.
Clinical outcome
Clinical outcomes were measured by GOS. In both the conventional pterional and pterional-subolfactory approach groups, all patients with unruptured ACoA aneurysms achieved good clinical outcome with GOS scores of 5. In the pterional-subolfactory group, postoperative CT revealed a cortical hemorrhage in 1 patient, and asymptomatic acute epidural hemorrhage in 1 patient. Cortical hemorrhage developed at the rectus gyrus removal site, and epidural hemorrhage developed at the operative approach side. However, neither patient developed neurological deficit due to hemorrhage, and the hemorrhages resolved spontaneously.
Among 34 patients with pterional-subolfactory approach, 23 patients had preoperative subarachnoid hemorrhage, and 20 patients (87%) made a good recovery (GR) followed by GOS higher than 4. Initial mental state for the other 3 patients was poor. Among them, families of 2 patients refused further treatment after initial operation, and the patients were discharged (Table 4).
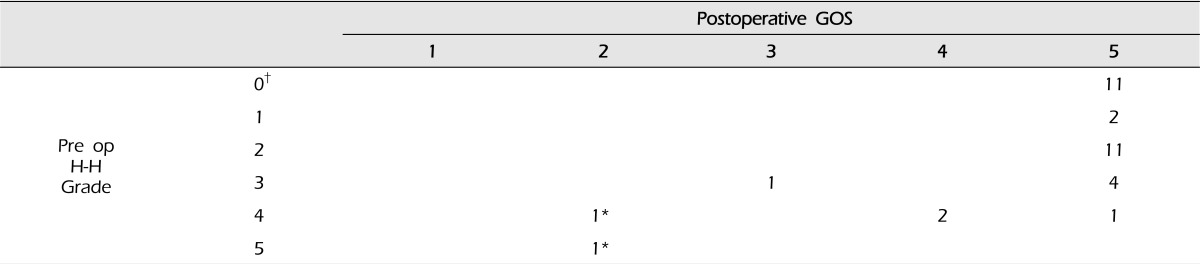
Conventional pterional approaches were performed for 13 patients with subarachnoid hemorrhage and 1 patient with unruptured high-positioned ACoA aneurysm. Twelve patients (92.3%) with subarachnoid hemorrhage achieved good clinical outcome with GOS higher than 4 (Table 3). Postoperative cerebral infarction was found in 2 cases with ruptured aneurysm.
Olfactory nerve function in unruptured ACoA aneurysm
Olfactory function was checked only for patients operated with unruptured ACoA aneurysm. Preoperative rupture of aneurysm with subarachnoid hemorrhage could alter the mental state of patients, and proper evaluation of surgical related olfactory dysfunction was not possible. Among 34 patients with pterional-subolfactory approach, 11 patients were treated for unruptured high positioned ACoA aneurysm. One patient (9.1%) complained of postoperative olfactory dysfunction in follow up (Table 5).
DISCUSSION
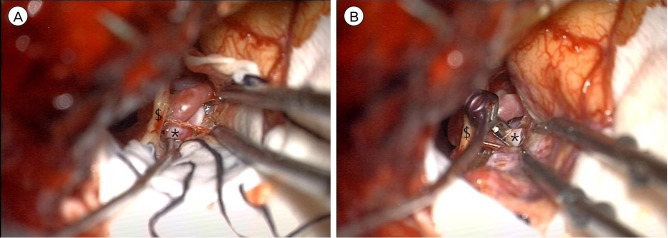
A rectus gyrus approach for anterior communicating aneurysm was first described by Kempe et al.3) in 1971. Since then, resection of the rectus gyrus has become the world-wide method for proper exposure of an anterior communicating aneurysm. In the standard method, the retractor is repositioned over the medial orbital gyrus just lateral to the olfactory nerve aiming toward the estimated level of the ACoA junction in the interhemispheric fissure. The pia of the gyrus rectus, immediately medial and parallel to the olfactory nerve, is cauterized and resected. This standard method provides a proper view of the anterior communicating aneurysm. In 1992, Horikoshi et al.2) reported clinical outcomes after rectus gyrus resection during conventional pterional approach. He concluded that resection of rectus gyrus helps to achieve safer aneurysm clipping without causing definite neurological sequelae affecting the postoperative outcome. However, with a highly positioned aneurysm, to retain the proper view of ACoA aneurysm, more retraction and elevation of frontal lobe is required and direct retraction injuries from the retractor can develop. Our pterional-subolfactory approach is different from the conventional pterional approach with removal of rectus gyrus in that we cauterize the pia of the rectus gyrus, immediately medial and inferior of olfactory tract after proper dissection of olfactory tract. In this way, we can preserve the olfactory tract most importantly, and achieve proper view and operation field for highly positioned ACoA aneurysm with no direct retraction needed (Fig. 1, 2). Our pterional-subolfactory approach requires no retractor to elevate frontal lobe.
In our study, we achieved good clinical outcome with no surgical related permanent complications in both conventional pterional approach and pterional-subolfactory approach group. The pterional-subolfactory approach resulted in shorter operation duration, and that difference was statistically significant. The olfactory dissection procedure might take additional operative time, but makes identification of aneurysmal neck easier for clipping.
In 1972, Pool demonstrated bifrontal craniotomy for ACoA aneurysms. Pool operated upon 60 ruptured ACoA aneurysms using low bifrontal craniotomy.7) He noted good clinical outcomes among good and fair risk group patients with 2.8% mortality and no surgical related complication. However, low bifrontal craniotomy can increase the possibility of postoperative infection due to frontal sinus opening and retraction injuries can develop during an interhemispheric approach due to bilateral brain retraction. Also, most neurovascular surgeons are more familiar with pterional craniotomy than interhemispheric approach with bifrontal craniotomy.
Anosmia is a well-known surgical related complication after ACoA aneurysm surgery. Hiroaki et al.1) performed a comparison study of anosmia after ACoA aneurysm surgery between the anterior interhemispheric and basal interhemispheric approaches in 1995. They reported 31% anosmia after anterior interhemispheric approach and 1.9% for basal interhemispheric approach. They concluded that frontal lobe depression and elevation during surgery may injure the olfactory nerve. Park et al.6) concluded olfactory dysfunction followed by pterional approach for cerebral aneurysms in 2009. Their study revealed high risk of olfactory dysfunction after pterional approach for ACoA aneurysm with 14.3% (10 of 70 patients). They concluded that direct pressure damage to the olfactory tract by spatula can be the possible reason for olfactory dysfunction. Olfactory dysfunction can pose a higher risk for older patients because of less elastic and more vulnerable olfactory nerves. In our study, we assessed olfactory nerve injury for unruptured aneurysm patients and found 1 case (9.1%, 1 of 11 patients) with pterional-subolfactory approach, very low compared to the literature.
The primary limitations of the present study are the retrospective design and the relatively small number of patients. In addition, olfactory dysfunction outcome was checked only for the unruptured aneurysm group due to preoperative mental status. Subarachnoid hemorrhage might have affected patient's preoperative mental status, and proper preoperative olfactory function evaluation was difficult. Also olfactory function of the conventional approach group was excluded in this study due to lack of old medical history. In the future, olfactory dysfunction outcome for both groups should be studied for comparison of both approaches.
CONCLUSION
In this study, we achieved excellent clinical outcome for both unruptured and ruptured ACoA aneurysms with no surgical related permanent complications except 1 case of olfactory nerve dysfunction. We concluded that pterional-subolfactory approach can be highly preferable for cases of high positioned ACoA aneurysm located higher than 10 mm above anterior clinoid process. Pterional-subolfactory approach can prevent olfactory bulb tearing, resulting in preservation of olfactory tract without any surgical complication. Also the subolfactory approach can provide wider and effective operation view with minimal retraction of brain. In conclusion, the pterional-subolfactory approach can be an alternative surgical approach for high positioned ACoA aneurysms.


 XML Download
XML Download