

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spontaneous intracerebral hemorrhage (sICH) accounts for 8-13% of all strokes and can result from a wide spectrum of disorders, including hypertension. In addition, compared to ischemic stroke or subarachnoid hemorrhage (SAH), primary sICH is more likely to result in death or major disability.2)3)
Several primary risk factors of sICH have been identified, including high blood pressure (BP), tobacco use, use of some drugs and/or alcohol, old age, and female gender.7)12)19)24) However, the relationship between seasonal variation and/or meteorological parameters and spontaneous SAH (sSAH) is unclear, and a few studies have attempted to demonstrate an association between the incidence of sICH and seasonality and/or meteorological parameters.1)6)11)
The aim of this study was to determine if any of the meteorological parameters, such as local temperature, atmospheric pressure, humidity, and daily temperature range, influence the risk of sICH in Incheon metropolitan city, which occupies a wide area of the western seacoast and many islands in the northwestern region of South Korea. Concurrently, we tried to determine whether the risk of sICH was associated with seasonality.
METHODS
We analyzed data of patients from a tertiary referral emergency center, which is the only level I regional emergency center in the northwestern area of South Korea. At this emergency center, almost all patients with acute sICH coming into this hospital's ER are admitted to the authors' department. The diagnosis of primary sICH was made by the universal standard methods. Electronic medical records and radiological findings for 708 consecutive patients admitted with a diagnosis of primary sICH from January 2008 to December 2010 were reviewed and analyzed. Secondary ICHs or those caused by trauma were excluded. Data on local temperature (℃), temperature range (℃), atmospheric pressure (hPa), and humidity (%) were collected with the help of Incheon Weather Station (latitude: 37°28'N, longitude: 126°37'E, elevation: 69 m).
The correlations between the estimated average monthly number of admissions due to sICH and local temperature, atmospheric pressure, humidity, and daily temperature range were estimated using autocorrelation analysis. The association of daily values of each weather parameter with the daily admission numbers of sICH was analyzed using a combination of correlation and time-series analyses. Autocorrelation analysis was used to measure the degree of self-correlation in the monthly admission numbers of sICH time series. The data were then analyzed statistically using SPSS 19 (IBM corp., Armonk, NY, USA).
RESULTS
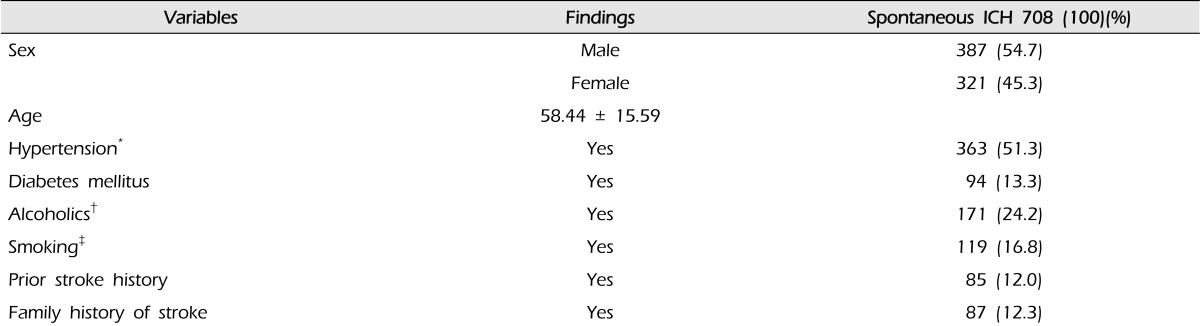
Table 1 shows the demographic and clinical characteristics of the patients with sICH enrolled in the present study. Included were 708 patients (387 [54.7%] men, 321 [45.3%] women), with an average age of 58.4 ± 15.6 years. Among the established risk factors for sICH, hypertension (51.3%) and alcoholism (24.2%; alcohol consumption more than twice per week) were the 2 most common risk factors in our study population.
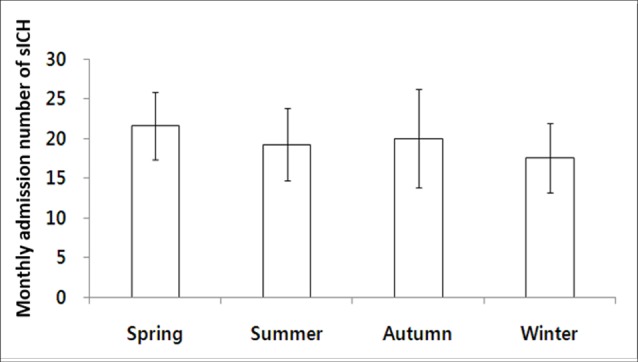
The association between the number of admissions due to sICH and season was not statistically significant (Fig. 1).
Fig. 2 shows the mean number of monthly admissions due to sICH during the study period. The time series of admissions shows a weak and rather irregular series of peaks and troughs, with no apparent annual or seasonal patterns. Results of autocorrelation analysis, which measured the degree of self-correlation in the monthly admissions due to sICH time series, are presented in Table 2 and Fig. 3.
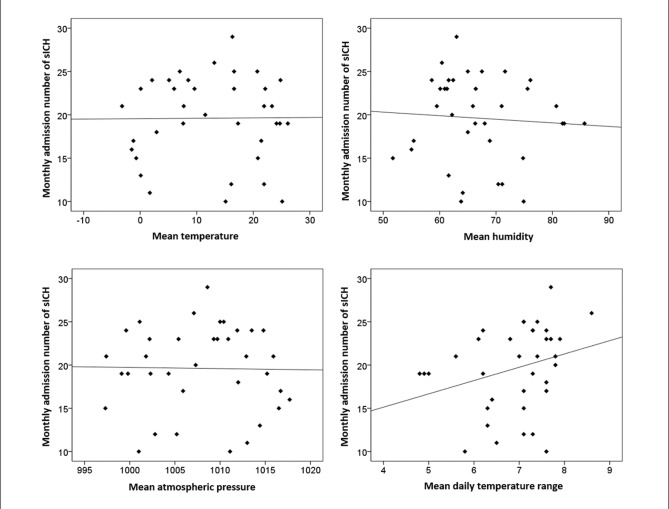
Despite the findings of no seasonality or annually recurring patterns in the average monthly admissions due to sICH, the possibility that the weather can influence the average monthly sICH-related admissions cannot be excluded. Therefore, the association of changes in the local temperature, atmospheric pressure, humidity, and daily temperature range with changes in the average number of monthly admissions due to sICH, during the study period for 3 years, was separately measured for each weather parameter (Table 2, Fig. 3).
Fig. 3 has plots depicting the association between the monthly sICH admission numbers and each weather parameter, and Table 2 describes the correlation analysis between them.
The local temperature (correlation coefficient [r] = 0.009, p = 0.959), local atmospheric pressure (r = -0.017, p = 0.923), local humidity (r = -0.068, p = 0.695), and local daily temperature range (r = 0.281, p = 0.097) were not associated with monthly admissions due to sICH. However, although chance findings could not be excluded, there was a tendency for the daily temperature range to be correlated with the number of sICH-related admissions to some degree.
DISCUSSION
Primary sICH is defined as a non-traumatic abrupt onset of severe headache and altered level of consciousness and/or focal neurologic deficit associated with a focal collection of blood within the brain parenchyma, as observed on neuroimaging or autopsy. It is not caused by rupture of cerebral aneurysms, arteriovenous malformations, hemorrhagic conversion of a cerebral infarction, or other causes of secondary ICH. The widespread availability computed tomography (CT) resulted in a dramatic change in our understanding of the incidence and risk factors of sICH.21)
During the past decades, diurnal and seasonal variations in the onset of primary sICH have been examined in many community- and hospital-based studies.4)10)13)22)
More recently, Shin et al.19) reported in their single institute-based study that winter was the most common season for the occurrence of sICH. Inagawa12) also stated in his population-based study that winter was the most common season for sICH among men belonging to a subgroup of younger patients (age ≤ 69 years) and a hypertension-induced subgroup; however, there was no significant seasonal pattern in women. Contrary to these reports, the present study revealed that, although there was no significant difference, spring was the most common and winter was the least common season for monthly admissions due to sICH (Fig. 1). While the exact reason for this difference remains unknown, we presume that it is due to differences in regional climate, such as the daily temperature range, and risk factors for sICH in the enrolled patients in each study. We further hypothesize that the high temperature range is more influential than the low absolute ambient temperature, as it can cause hemodynamic instability and eventually lead to sICH.
BP, blood viscosity, serum lipid levels, sympathetic nervous system activity, blood clotting time, and fibrinogen levels are affected by season and weather and could alter the risks of a stroke.9) Our study partially supports the concept that changes in meteorological parameters drive the relationship between weather and sICH. In contrast to our finding of winter being the least common season for sICH-related admissions, cold exposure is thought to increase BP by activating the sympathetic nervous system, and the seasonal influence on BP is the highest in the winter.15)18)25)
However, the relevant physiological mechanisms involved in the above-mentioned phenomenon remain unknown. The most physiologically significant alteration associated with low temperatures is an increase in BP. As the temperature decreases, BP increases and becomes more labile. This effect is particularly true in unacclimatized humans who are transitioning from normal temperatures to very cold or freezing temperatures. Therefore, lower temperatures are associated with increases in the risk of coronary artery disease and ICH.5)8)16)
Other potential etiological factors that could increase the risk of sICH include abrupt changes in physical activities and health-associated behaviors such as smoking, heavy alcohol consumption, and the physiologic response to exercise.9)14)17)20)
The present study has several limitations. First, being a retrospective study, it has potential analytic limitations for some clinical variables and characteristics such as risk factors for sICH, including previous/present medication and/or comorbidities (such as antiplatelet administration, amyloid angiopathy, prior cerebral infarction and hypercholesterolemia) that might directly affect the occurrence and precise onset time of sICH. Second, Incheon metropolitan city has a very long coastline and many islands, and the climate parameters used in our study were recorded at the Incheon weather station, not on the site where the sICH occurred. This might influence the association between the occurrence of sICH and meteorological parameters. Third, although patients were enrolled from the only level I regional emergency center within the territory of Incheon metropolitan city, because this is a single hospital-based, and not a population-based study, the true local incidence of sICH and its association with the local meteorological parameters are still unknown.
CONCLUSION
In our study, the number of admissions due to primary sICH did not vary significantly seasonally or in association with the local meteorological parameters. However, the daily temperature range tended to affect the number of admissions due to sICH. Although our results were not statistically significant, prospective multi-institutional or global studies that include hospitals located in regions with varying latitudes and seasonality should be conducted to investigate the association between sICH incidence and meteorological parameters such as daily temperature range.


 XML Download
XML Download