

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Moyamoya disease (MMD) is characterized by a chronic progressive steno-occlusive change of the distal internal carotid artery and abnormal development of a fine vascular network (Moyamoya vessels) at the base of the brain. Takeuchi and Shimizu11) had initially reported this disease in 1957, followed by Suzuki11) in 1969 who named the disease as Moyamoya (the Japanese word for puff of smoke).
The disease was initially known to be endemic where it was limited to Japan but is now found worldwide.4-9)12)15) Several studies have indicated a high prevalence of MMD in Asian countries, particularly in Japan, Korea, and China.2)8)9) Japan has the highest outbreak of illness frequency, followed by Korea and China. It appears that these countries have higher incidences than other areas. The national prevalence of MMD in Japan is well-documented.7)13) Until this investigation, the epidemiology of MMD in Korea has not been reported.
We reviewed the National Health Insurance Corporation (NHIC) data to study the epidemiological features of MMD in Korea.
MATERIALS AND METHODS
The authors requested data from the NHIC of MMD patients who were treated from 2004 until 2008 in Korea. The following measures were investigated: age, gender, incidence, and prevalence. The data in this study were standardized based on data of the South Korean population in 2004-2008, which was provided by Statistic Korea.
In the present investigation, these data gathered from NHIC may not adhere strictly to the criteria for MMD proposed by Yonekawa et. al.14)
And we could not gather detailed data including symptoms, diagnostic and treatment methods of the MMD.
RESULTS
Incidence and Prevalence
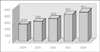
The NHIC data revealed that in 2004, 2,539 MMD patients were treated in Korea, representing a prevalence rate of 5.2 per 100,000 people. The respective numbers of patients and prevalence rate were 2,987 and 6.3 in 2005, 3,429 and 7.0 in 2006, 4,051 and 8.6 in 2007, and 4,517 and 9.1 in 2008, representing an annual increase of 15%. In 2008, 466 people were newly diagnosed with MMD, representing an incidence rate of 1 per 100,000 persons. The prevalence of MMD in Korea increased from 5.2 per 100,000 in 2004 to 9.1 per 100,000 in 2008 (Fig. 1, 2).
Gender differences
Four thousand five hundred seventeen Korean patients were treated in 2008. The gender balance was 1,547 men (34%) and 2,970 women (66%). The incidence rate for women was 1.94 times higher than men were.
Age distribution
The age distribution is displayed in Fig. 3. There is a bimodal peak pattern, first on teenagers (10-19 years old) and second among those in their forties (40-49 years old).
DISCUSSION
MMD was first described in Japan, and originally considered a disease that predominantly affected Asian populations. Its prevalence is highest in Japan, followed by Korea and China.8) In Japan, four national surveys were conducted: 1986, 1990, 1995, and 2003.7) In 2003, the total number of patients treated in Japan was estimated at 7,700 and the annual rate of newly diagnosed cases in 2003 was 0.54 per 100,000 population.
The estimated prevalence of MMD in Japan has almost doubled during the most recent decade where data is available (3,900 in 1994 and 7,700 in 2003).7) In Korea, MMD was first reported in 1969, based on case reports of hemangiomatous malformation of the brain.2)
In Korea, two co-operative studies on MMD patients treated at several neurological institutes were reported. However, to date, the national epidemiological features of MMD in Korea have not been reported.2)3)5) This is the first study to report the Korean national epidemiology of MMD.
The authors obtained data from the NHIC on MMD patients who were treated from 2004 to 2008. Almost all Koreans are affiliated with the NHIC. These data included both symptomatic and asymptomatic cases.
In 2008, 466 people were newly diagnosed with MMD, representing an incidence rate of 1 per 100,000 persons. The prevalence of MMD in Korea has increased from 5.2 per 100,000 in 2004 to 9.1 per 100,000 in 2008. The annual increase may reflect both an actual increase in new cases and an increased detection of asymptomatic existing cases due to an improved diagnostic capability and developing brain check-up system. Increasing numbers of MMD cases have been reported worldwide.1)7)15) In Japan, the prevalence and annual rate in 1994 were 3.16 and 0.35 per 100,000 people and in 2003, it was reported as 6.03 and 0.54 respectively.7) The prevalence rate almost doubled in 10 years because of the increase in the occurrence rate. The higher detection rate and prevalence of MMD in Japan may have contributed to the increase in newly diagnosed cases. After an induction of recently developed noninvasive diagnostic tools, asymptomatic MMD is being diagnosed more frequently.7)
In Korea, the prevalence rate of the MMD was 6.03 per 100,000 in 2003. It rose to 5.2 per 100,000 in 2004 and 9.1 per 100,000 in 2008. Thus, the prevalence of MMD in both Japan and Korea is similar.
The well-known specific features of MMD are a bimodal pattern of age distribution and female prevalence. This study revealed a bimodal age distribution where the highest was observed among teenagers, followed by those in their forties. There was a higher incidence in women than in men (1.94 times). National figures for MMD in China have not been reported, but there is data on the epidemiological and clinical features in Nanjing, a provincial capital city.9) The annual average detection rate was 0.43 per 100.000 and the prevalence rate was 3.92 per 100,000. This was lower than the prevalence of 6.3 found in Japan and 5.2 found in Korea, but similar to Taiwan.4) MMD has been observed throughout the world and it affects individuals from different ethnic backgrounds.9) But it is rarely observed among Americans and Europeans. A recent European study has reported an incidence of approximately 1/10 th of that in Japan.15) Studies in the United States suggest an incidence of 0.086/100,000 persons.12) Compared to Whites, ethnicity-specific incidence rate ratios were 4.6 for Asian Americans, 2.2 for African Americans, and 0.5 for Hispanics.12)
Based on the Japanese national data, the prevalence rate of MMD between Japan and Korea are similar.
CONCLUSION
In conclusion, the prevalence rate of MMD was 5.2 per 100,000 in 2004 and it increased at a rate of 15% annually through 2008. This increases the Korean population prevalence to 9 per 100,000. The Japanese prevalence rate of the MMD in 2003 was 6.03 in 100,000. As such, the prevalence rate of MMD between Japan and Korea is similar. And their prevalence is highest among the world.


 XML Download
XML Download