

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spontaneous intracerebral hematoma (sICH) occurs as a result of stroke and is characterized by the spontaneous extravasation into the parenchymal tissue of the brain.15) After the initial hematoma, hematoma expansion and perihematoma edema can result in secondary brain damage and a poor prognosis.7) Potential outcomes include prolonged or permanent neurological dysfunction, with neurological deficits evolving over the course of minutes or hours, and persisting for days or weeks. Rapid hematoma enlargement is one of the definite prognostic factors and is often observed in cases involving sICH.16) Furthermore, the outcome of surgical management for huge sICH was associated with a high mortality.6) Rapid spontaneous reduction of a traumatic acute subdural hematoma (SDH) has been frequently reported. However, it was rarely reported that rapid spontaneous reduction occurred in large volume of sICH. In this study, we describe a patient with a rapid spontaneous decrease in the volume of the hematoma and discuss the mechanism involving the spontaneous rapid reduction.
Go to : 
CASE REPORT
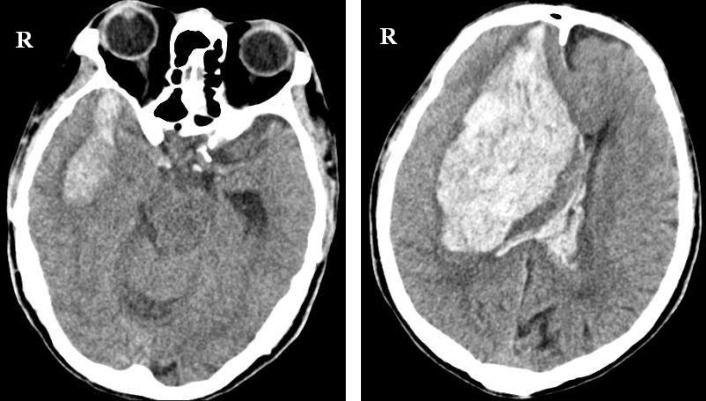
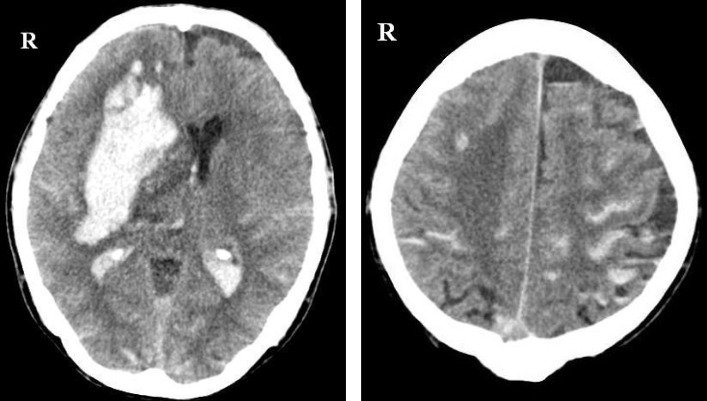
A 73-year-old man was admitted with mental deterioration. He displayed a semi-comatose mentali ty, with a Glasgow Coma Scale (GCS) score of 6 (E1 V2 M3). His pupils were anisocoric with left pupil dilated and did not reflex to light. The initial brain computed tomography (CT) revealed a massive sICH on the right basal ganglia which extended into the frontal lobe, about 210 cc, as well as subarachnoid and intraventricular hemorrhages with a severe midline shift of 2.2 cm (Fig. 1). An emergency decompressive craniectomy and removal of sICH were planned to relieve the subfalcial herniation, but was not performed due to the refusal of the patient's family. Therefore, we decided to treat with a conservative therapy. Follow-up brain CT after 16 hours demonstrated remarkable decrease in the volume of sICH to about 125 cc and showed the decrease of the mass effect and the increase of subarachnoid hemorrhages and intraventricular hemorrhages (Fig. 2). Based on this finding, we planned a surgical procedure for removal of the hematoma and control of intracranial pressure, with consent from the patient's family.
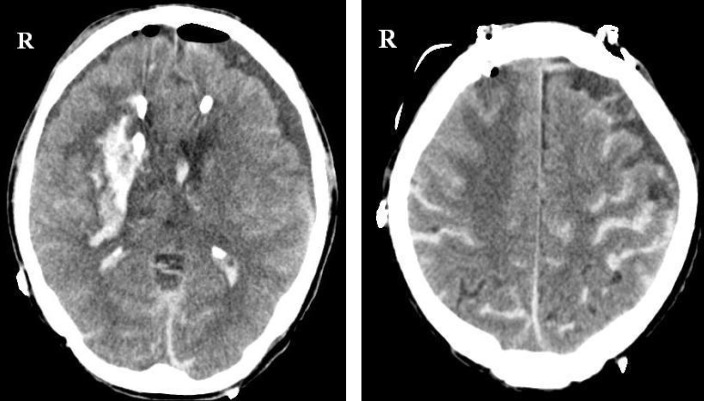
We performed the stereotactic aspiration of sICH and insertion of drainage catheter under general anesthesia. The postoperative CT revealed a remarkable decrease in the volume of the hematoma compared with that of hematoma in the initial CT imaging (Fig. 3). However, there was no improvement in the patient's condition. About a month later, the patient was transferred to a rehabilitation facility as remaining in a stuporous state, with a GCS score of 8 (E2 V2 M4). At the neurologic examination 6 months after initial insult, the patient remained in a bed-ridden state without improvement.
Go to :
DISCUSSION
A large volume of sICH is a devastating disease with high rates of mortality and morbidity.7) The classic presentation of sICH includes the sudden onset of a focal neurological deficit that progresses over minutes to hours with accompanying headache, nausea, vomiting, decreased consciousness, and elevated blood pressure.5) The hematoma volume is the most potent predictor of mortality and poor functional outcome in patients with sICH.17) Furthermore, acute expansion of the hematoma within an hour to a day, has been reported as a cause of severe neurologic deterioration and death.14)
In our patient with a huge sICH exhibited a rapid spontaneous reduction in the volume of the hematoma over a very short period of time. The initial brain CT revealed a large basal ganglia hematoma and signs of impending subfalcial herniation. Fortunately, follow-up brain CT 16 hours after initial insult showed a remarkable decrease of the hematoma volume. However, the patient in our study had a large hematoma that decreased in volume within a short time period without improvement of the symptoms attributed to the hematoma.
The rapid expansion of a sICH has been frequently reported.1)14) However, we found limited reports describing the rapid spontaneous decrease in the volume of the hematoma observed in ICH.4) A patient with a petrous bone fracture after trauma showed a spontaneous cure of ICH by drainage into the middle ear.4) However, it was a rare case of traumatic ICH unlike our case. In our case, the ICH was not related to head trauma, so it appears to have been a large hematoma which decreased spontaneously.
However, rapid spontaneous resolution and a decrease in the size of the traumatic acute SDH have frequently been reported.2)3)8)9)11-13)19) The pathophysiology of this phenomenon is not well understood, and many hypotheses have been proposed. Four mechanisms for the rapid resolution of the hematoma have been proposed; dilution and wash out of the hematoma by cerebrospinal flow (CSF) after tearing of the arachnoid membrane; compression and redistribution of the hematoma by acute brain swelling; redistribution of the hematoma through skull fractures; and redistribution of the hematoma to the spinal subdural space.2)3)9-13)18)19) However, the clear mechanism for spontaneous resolution of acute SDH was not identified, especially in that of sICH.
In our case, the patient presented with a basal ganglia hematoma with a margin very close to the subarachnoid and intraventricular spaces. We proposed that pressure from the massive hematoma caused rupture of the adjacent cortical surface and pia mater, resulting in migration of the hematoma into the subarachnoid spaces. In the same way, that resulted in the rupture of the ependymal lining of ventricle and so migration of hematoma into ventricular spaces. On the follow-up brain CT, we found the increased volume of subarachnoid hemorrhages and intraventricular hemorrhages. This finding may support the hypothesis of dilution and wash out of the hematoma by CSF after tearing of the arachnoid membrane. The hematoma mixed with CSF may be a clue in the redistribution process.2)8)11)13)18)20) CSF liquefies the hematoma and the blood clots are redistributed to the subarachnoid and ventricular spaces.11) In the spontaneous rapid reduction of ICH, we suggest that the hematoma mixed with CSF also may be a same mechanism in the distribution process and CSF liquefies the hematoma and the blood clots are redistributed to the subarachnoid and ventricular spaces like several report on spontaneous resolution of acute SDH.
Go to :
CONCLUSION
This is a very rare case in which a rapid spontaneous reduction occurred in large volume of sICH. The mechanism involving the rapid decrease of the hematoma is presumed to occur through redistribution in brain atrophy, compression effect from the increased intracranial pressure and dilution through a wash out by the cerebrospinal fluid.
Go to :
 XML Download
XML Download