

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In the dental field, cone-beam computerized tomography (CBCT) has become more prevalent in the past decade.1 One of the advantages of CBCT is that it provides an accurate 3-dimensional image with good resolution that helps facilitate the diagnosis. In addition, it exposes the patient to less radiation than traditional CT scans.123
Soft tissue calcification is a pathological condition in which calcium and phosphate salts are deposited in the soft tissue organic matrix.4 Soft tissue calcifications are classified as dystrophic, metastatic, and idiopathic. In the dystrophic type, which is the most frequent, calcification occurs in damaged tissue, and the affected individual's calcium and phosphorus levels tend to be normal. The metastatic type is associated with disturbances in calcium and phosphorus metabolism, such as in cases of hyperparathyroidism and chronic renal failure.5 The idiopathic type is a rare disorder in which the underlying cause of the calcification is not identifiable, and serum calcium and phosphorus levels are normal. It is diagnosed after ruling out all other potential calcification types and their etiologies.6
Eustachian tube calcification is associated with age-related histopathological changes, and refers to the accumulation of small granules of calcium phosphate and calcium carbonate, primarily in the intracellular substance of the cartilage. With time, as these granules coalesce and enlarge, nutrient supply to the cartilage cells is significantly diminished, which compromises the proper function of the cartilage.78
The Eustachian tube is defined as a narrow tube that extends from the middle ear to the nasopharynx,9 with an approximate length of 43 mm in an adult.10 The tube consists of two parts: the bony part, which is mainly formed by the petrous part of the temporal bone, and the fibrocartilaginous part that is attached to the base of the skull via suspensory ligaments.11 The main functions of the Eustachian tube are to equalize atmospheric pressure in the middle ear, particularly during activities such as swallowing. It also allows the mucociliary clearance of the middle ear, and protects the ear from undesirable sound.12
To the authors' knowledge, no previous study has reported the diagnosis of Eustachian tube calcification using CBCT. However, a case diagnosed using multidetector CT was reported in the literature.13 The purpose of this article is to present an unusual case of Eustachian tube calcification noted on CBCT imaging.
Case Report
A 67-year-old woman presented for dental treatment, specifically implant placement. Her past medical history included ablation of a hypertrophic thyroid and subsequent treatment with Synthroid medication (AbbVie Inc., North Chicago, IL, USA), depression that was treated with Klonopin (Genentech, South San Francisco, CA, USA), and intermittent soreness in the muscles near her ears. No history of diabetes or renal insufficiency was noted, and the patient denied any other significant medical history. Neither her family nor social history was significant.
CBCT was obtained for preoperative planning for implant placement and to evaluate and assess the pre-implant region. A high-resolution scan (90 microns) with a medium field of view was obtained using a Carestream CS9300 apparatus (Carestream Dental LLC, Atlanta, GA, USA). The CBCT volume was referred to the Department of Oral and Maxillofacial Medicine and Diagnostic Sciences for further review.
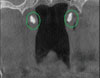
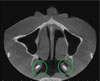
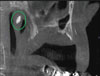
The volumetric scan was evaluated by a board-certified oral and maxillofacial radiologist. The study revealed an edentulous region in the region of interest where implants were planned. Additionally, the volume showed incidental findings of 2 distinct hyperdense regions in the cartilaginous portion (torus tubarius) of the Eustachian tubes. Figure 1 shows bilateral homogenous hyperdense regions in the coronal slice. The left calcification appears to have been larger than the one on the right side. Each calcification spanned approximately 2.5 mm×5 mm. Figure 2 depicts an axial slice, showing hyperdense regions in the torus tubarius of the Eustachian tube. A sagittal view showing calcification on left side of the torus tubarius region is depicted in Figure 3. Volume rendering showing the bilateral calcifications, which are delineated by circles, is presented in Figure 4. Figure 5 depicts the anatomical relationships of the Eustachian tube with its surrounding structures.
Discussion
We report a case of Eustachian tube calcification that was noted as an incidental finding. To the best of the authors' knowledge, this is the first such case to have been observed using CBCT volumetric imaging.
The Eustachian tube is one of the most complicated structures in the human body; it has a complex anatomy with incompletely understood physiology, and pathological states within the Eustachian tube are relatively infrequently examined. The Eustachian tube is not just a tube, but an organ consisting of a lumen with mucosa, cartilage, soft tissue surroundings, peritubular muscles, and bony support.1214 The Eustachian tube is lined with a pseudostratified ciliated columnar-lined, S-shaped passage connecting the middle ear to the nasopharynx.15 The average length ranges between 31 and 38 mm in adults.11 Anatomically, the Eustachian tube is divided into osseous, junctional, and cartilaginous portions, with the osseous portion being nearest the middle ear and the cartilaginous portion running between the greater wing of the sphenoid and the petrous portion of the temporal bone.15 The cartilage provides structural support to the Eustachian tube, while still allowing mobility,13 and its function is intimately related to the structure, composition, and attachment of the cartilage.12 The Eustachian tube has 3 physiologic functions: 1) pressure regulation, 2) protection of the middle ear from excessive sound pressure, and 3) drainage of nasopharyngeal secretions.15 The anatomy of the Eustachian tube is depicted in Figure 5.
The fibrous cartilage surrounding the Eustachian tube takes the shape of an inverted J, with the medial lamina on the medial aspect of the tube and the lateral lamina on the superolateral aspect,7 as shown in Figure 5. Ostmann's fat pad lies between the tensor veli palatini muscle and the Eustachian tube lumen, and it closes the lumen by exerting pressure on the lumen.7 At rest, the lumen of the Eustachian tube is closed, and it opens during swallowing to equilibrate positive pressure via 4 muscles: the tensor veli palatini, levator veli palatini, tensor tympani, and the salpingopharyngeus.16
Although clinical evidence of Eustachian tube calcification is almost nonexistent, Morshedi and Mafee published the first and only documented case in 201113 and more recently Buch et al. retrospectively reviewed torus tubarius calcifications.8 Calcium deposition has been shown to occur with aging and various pathological processes, and is more frequently found in the elderly.817 Calcification begins when small granules of calcium carbonate and calcium phosphate are deposited intracellularly and then into the surrounding matrix. The small granules increase in size, merge together, and cause cartilage to become brittle.7
Heterotrophic calcification occurs when calcium salts, mainly calcium phosphate, are deposited in soft tissue instead of bone.18 Heterotrophic calcifications are classified as dystrophic, idiopathic, or metastatic. Dystrophic calcifications are caused by dead, diseased, and damaged tissues, and therefore are contained to the area of injury. Idiopathic calcifications are calcium deposits in tissues despite average calcium and phosphate levels, as exemplified by phleboliths. Higher levels of calcium seen in hyperparathyroidism, or increased levels of phosphate noted in chronic renal failure, cause calcium and phosphate to precipitate into healthy, normal tissues. These calcifications are known as metastatic and commonly occur in a symmetrical, bilateral pattern.18 Although serum calcium and phosphate levels were not recorded for the patient in question, the bilateral, symmetric appearance and lack of tissue damage led the authors to believe that her Eustachian tube calcifications were metastatic in nature.
Although uncommon, it has been proposed that ossification or calcification of the Eustachian tube cartilage may result in loss of elastic function and increased rigidity, preventing effective opening or closing of the Eustachian tube.7 Takasaki et al. reported the presence of numerous calcified cells in the Eustachian tube cartilage through histopathological testing, and they speculated that calcifications decrease the elasticity of the cartilage and alter its function.7 Furthermore, calcification has been associated with fatty infiltration of the tensor veli palatini muscle, which may additionally contribute to Eustachian tube dysfunction.13 The patient reported no positive signs of Eustachian tube dysfunction such as muffled hearing, tinnitus, popping sounds, ear pressure, or abnormal hearing; however, the patient had infrequent muscle soreness in the ear region, which could be attributed to failure of the Eustachian tube to provide proper clearance of middle ear secretions and pressure equalization. The cartilaginous portion of the Eustachian tube is elastic in nature and calcifications reduce its opening and closing effectiveness.13
Takasaki et al. noted a link between chronic renal failure (CRF) and cartilage ossification,19 but the patient's report lacked CRF in her health history, leading us to suspect an alternative cause of calcification in our case. Takasaki et al. also found a correlation between the number of calcified chondrocytes in the medial lamina and lateral lamina and age,7 suggesting higher rates of Eustachian tube calcification in elderly patients. This may be relevant for the case of this 67-year old patient. Although Eustachian tube calcifications caused directly by hyperthyroidism have not been documented, hyperthyroidism has been known to cause hypercalcemia. The patient suffered from hyperthyroidism before undergoing ablation 4 years ago, and this condition may have caused elevated serum calcium levels, and ultimately a slow accumulation of metastatic calcifications in the Eustachian tube. Further investigation of this possibility is needed.
In summary, the current case report described an uncommon variant of Eustachian tube calcification, which has significant didactic value because such cases are seldom illustrated in textbooks. This case also illustrated the importance of having CBCT scans ordered for restorative purposes evaluated by a board-certified oral and maxillofacial radiologist.


 XML Download
XML Download