

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Magnetic resonance imaging (MRI) is a reliable method of displaying both soft and hard tissues for the classification of internal derangement 1234 because magnetic resonance (MR) images using high magnetic field strength and small surface coils provide excellent visualization of the temporomandibular joint (TMJ),1 particularly for assessing disc position and configuration, and degenerative bony changes.5
Sagittal and coronal MR images have become a reference standard for the diagnosis of internal derangement of the TMJ. However, the results obtained from MR images are influenced by diagnostic criteria and observer performance, as well as MRI techniques.6 The combination of sagittal and coronal images is useful for TMJ evaluation. This combination yields higher accuracy than sagittal images alone in determining the disc position and configuration, and osseous changes of the TMJ. Sagittal and coronal MR images have been found to be 95% accurate for assessing disc position and shape, and 93% accurate for assessing osseous changes.7
The detailed criteria for identifying normal and abnormal joints provide an opportunity for greater sensitivity in detecting internal derangement and characterizing progressive changes of the TMJ.6 The normal TMJ disc has a biconcave shape, with the thin intermediate zone in the 10 o'clock position and the narrowest inter-bony distance and posterior band of the articular disc located above the apex of the condylar head, or the 12 o'clock position.8
Internal derangement of the TMJ is defined as an abnormal positional relationship of the articular disc, mandibular condyle, and the articular eminence, which can interfere with smooth joint movement.9
Morphological changes of the TMJ disc have been recognized as an important feature of internal derangement and as a cause of functional impairment.10 Degenerative changes of the disc are influenced by the degree and type of disc displacement, and the more advanced the internal derangement, the greater the deterioration of the disc configuration.11
MRI has been found to show adequate agreement between the clinical examination and the imaging findings.212 The most common clinical symptoms of internal derangement of the TMJ are pain, muscle tenderness, joint sounds (clicking or crepitation), and limited opening of the jaw. However, the relationship between the MRI evidence of internal derangement and the occurrence of pain remains unclear. Temporomandibular disorder (TMD) is diagnosed by a combination of clinical and diagnostic imaging findings. Determining the precise relationship between pain and internal derangement requires a systematic correlation of clinical signs and symptoms with the results obtained from MR images.613
Tasaki et al.7 observed internal derangement in one or both joints in nearly one-third of asymptomatic volunteers. This observation is consistent with other studies of asymptomatic volunteers.914 According to the study of Emshoff et al.,9 TMJ pain was related to internal derangement visualized using MRI. However, MRI variables might not be the dominant factors for defining TMJ pain occurrence.
In previous studies, contradictory findings have been reported regarding the relationship between pain and internal derangement. Some studies concluded that internal derangement could be accurately diagnosed using well-defined clinical examinations and criteria.1516 However, others concluded that clinical examinations were insufficiently reliable to determine disc position.17181920
The aim of this study was to determine the relationship between the evidence of internal derangement observed on MRI and TMJ pain, including spontaneous and provoked pain, in TMD patients.
Materials and Methods
The study included 356 TMD patients (712 TMJs) who visited Chonbuk National University Dental Hospital, Korea, with TMJ pain between 2008 and 2015. Their dental records were investigated and MRI was performed with the written consent of the patients.
The inclusion criteria were the availability of appropriate MR images and the presence of spontaneous or provoked pain on one or both TMJs. Spontaneous pain was defined as being present when patients referred to pain in their history. The patients with provoked pain were classified into 3 groups: those with pain on palpation (G1), those with pain on mouth opening (G2), and those with pain on mastication (G3). The severity of pain was assessed by a visual analog scale (0–10).
The patients' MR images were acquired using a 1.5-T scanner (Symphony, Siemens, Olangan, Germany) with a 7.5-cm surface coil. A 3-mm section thickness with a 140-mm field of view and spin-echo multi-section images were used. For T1-weighted images, the repetition time and echo time were 510-520 ms and 11-15 ms, respectively, and for T2-weighted images the repetition time and echo time were 2410-2740 ms and 40-107 ms, respectively. Eighteen paracoronal and 11 parasagittal images were obtained. All TMJs were evaluated to detect the presence of joint effusion on the MR images.
The MR images were evaluated independently by 2 experienced oral and maxillofacial radiologists at 2 different times. When there was disagreement, a final assessment was reached by consensus.
Statistical analysis was performed by the chi-square test using SPSS version 12.0 (SPSS Inc., Chicago, IL, USA). For comparisons of TMJ pain and internal derangement, P values <.05 were considered to indicate statistical significance.
Results
Table 1 shows the age and gender distribution of the study subjects. The subjects comprised 356 TMD patients (83 males and 273 females). The ratio of males to females was 0.3. Of the 356 TMD patients who had experienced TMJ pain, the second and third decades predominated (67.7%). The mean age of those who experienced pain was 25.8 years (range, 11–74 years).
Table 2 shows the distribution of TMJ pain in the TMD patients according to the site. Of the 356 right TMJs examined, spontaneous pain was found in 292 joints (34.3%), provoked pain on palpation in 162 (19.0%), pain on mouth opening in 179 (21.0%), and provoked pain on mastication in 219 (25.7%). Of the 356 left TMJs examined, spontaneous pain was found in 291 joints (34.3%), provoked pain on palpation in 160 (18.9%), pain on mouth opening in 181 (21.4%), and provoked pain on mastication in 215 (25.4%).
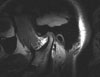
Table 3 describes the findings regarding the relationship between spontaneous pain and internal derangement in the TMJs. Figure 1 shows a normal disc position, with the posterior band of the disc located superiorly to the condyle. The disc showed a biconcave configuration, with the thin intermediate zone in the 10 o'clock position. Figures 2A and 2B show disc displacement with reduction. A T1-weighted image in the closed mouth position shows mild anterior disc displacement and a T2-weighted image in the open mouth position shows a recaptured disc. Figures 3A and 3B show disc displacement without reduction. A T1-weighted image in the closed mouth position shows anterior disc displacement and a T2-weighted image in the open mouth position shows anterior disc displacement relative to the condyle.
No correlation was found between spontaneous pain and internal derangement in TMD patients (P=.067).
Table 4 presents the relationship between provoked pain on palpation and internal derangement in TMJs. No correlation was found between provoked pain on palpation and internal derangement in TMD patients (P=.498).
Table 5 demonstrates the relationship between provoked pain on mouth opening and internal derangement in TMJs. Provoked pain on mouth opening was found to be correlated with internal derangement in TMD patients (P=.006).
Finally, Table 6 presents the relationship between provoked pain on mastication and internal derangement in TMJs. No correlation was found between provoked pain on mastication and internal derangement in TMD patients (P=.266).
Discussion
Anterior disc displacement is a form of intracapsular dysfunction that leads to degenerative changes in the disc and articular surfaces, as well as in the retrodiscal tissues.11 Most frequently, the TMJ disc is displaced anteriorly, but it can also be displaced medially or laterally.
On MR images, the relatively low signal intensity of the normal TMJ disc can be distinguished from that of the surrounding soft tissues. A distinct demarcation between the posterior band of the disc and the posterior attachment can be observed, and the normal disc has a biconcave configuration.811 Deformation of the disc is frequently found, and the normal biconcave shape seems to change as a result of disc displacement. The thickening of the posterior band, particularly biconvex deformation of the disc, can be clearly seen on MR images. Using MRI, anterior disc displacement without reduction was found to be the most common form of internal displacement of the TMJ, accounting for 54%–59% of TMJ derangements.21 Additionally, typical anterior disc displacements may be rotated and partially displaced medially or laterally. Miller et al.22 reported that the discs were thickened and deformed in all cases of anterior disc displacement without reduction. The exact contribution of the disc to the mechanics of the TMJ remains poorly understood.152324 However, Campos et al.24 reported that the main articular alterations were disc displacement and degenerative changes in both the soft and hard tissues of the TMJ.
The causes of pain in TMD patients are not clearly understood. The correlation between joint pain and disc position might have multiple causes.92526 TMJ symptoms include pain, clicking sounds and limitation of jaw movement, although not all are the result of internal derangement of the joint.8 Pain symptoms frequently arise in patients with TMJ internal derangement. According to Murakami et al.,27 the MRI detection of a high signal intensity in anterior disc displacement without reduction was not found to be correlated with TMJ pain, but chewing pain and joint effusion were positively correlated with anterior disc displacement without reduction. Disc displacement without reduction was usually associated with the absence of joint sounds, the presence of TMJ pain and muscle spasms, and limited jaw opening. In general, previous studies indicate that it might not be possible to determine the causes of TMJ pain through a clinical examination alone.
MRI can be used to evaluate internal derangement if a clinical examination cannot determine the true position of the disc.28 In previous studies, the diagnostic criteria and classification systems for disc position have varied. Some studies have used previously developed systems1729, while several other studies have used their own classification systems.151630 Although Tasaki et al.7 presented a classification system that utilized 10 categories, other studies173132 have reported only 2 or 3 categories being used within a single system.
Many authors have reported that anterior disc displacement was an important source of joint pain.242633 Anterior disc displacement without reduction might lead to more mechanical stress, and stretch the posterior disc attachment and joint capsule to a greater extent than anterior disc displacement with reduction, causing more painful joints.24 Clinical and MRI investigations of disc morphology have demonstrated significant differences between symptomatic and asymptomatic subjects, and between joints with internal derangement and normal joints.34 However, Sano et al.35 found that the majority of asymptomatic individuals showed a normal disc position, with only one-third exhibiting anterior disc displacement. In previous studies, disc displacement was observed in 30% of asymptomatic volunteers and a normal disc position was observed in 13.8% of symptomatic patients.715 The number of healthy individuals with disc displacement ranged from 17.5% to 35.0%. Ohlmann et al.36 reported that internal derangement was not significantly correlated with the presence of TMJ pain. Some authors have demonstrated that anterior disc displacement of the TMJ does not necessarily correlate with joint pain.373839 Moreover, studies of the relationship between sideways disc displacement and joint pain have yielded controversial results.1240
The clinical parameters of pain, muscle tenderness, and a clicking sound of the TMJ were correlated with the MRI findings relating to disc shapes even in biconcave discs.41 It was reported that anterior disc displacement, particularly anterior disc displacement without reduction, using pseudo-dynamic MRI, was an important source of TMJ pain.42 High signal intensity and prominent enhancement of the posterior attachment on fat-saturation T2-weighted imaging and dynamic MR imaging with contrast media were closely correlated with the severity of TMJ pain.43
Larheim et al.44 reported that partial disc displacement in the TMJ generally did not seem to be associated with clinical symptoms. Internal derangement in asymptomatic volunteers was less prevalent, less frequently bilateral, and more often partial than in patients with TMJ pain, who more frequently presented with bilateral and complete disc displacement.
Kumar et al.45 showed that disc displacement identified using MRI correlated closely with the presence or absence of clinical signs and symptoms of TMDs, with a high sensitivity and specificity (90% and 83.3%, respectively). A significant relationship was found between the presence of TMJ pain and MRI diagnoses of anterior disc displacement without reduction. Emshoff et al.46 reported a correlation between TMJ pain associated with anterior disc displacement without reduction and MRI diagnoses of internal derangement. Moreover, Marguelles-Bonnet et al.47 reported a highly significant correlation between MRI findings and the clinical data for all categories of derangement. Therefore, the clinical diagnostic criteria for anterior disc displacement without reduction can be used as a reliable method for predicting MRI diagnoses. However, in other studies, the clinical presence of pain was not a reliable indicator of internal derangement on MRI in patients with TMJ pain.3248
As described in a previous study,6 spontaneous pain was defined as pain upon awakening in the morning or pain in the afternoon not related to a specific stimulus, while provoked pain was defined as pain upon movement of the jaw or in response to a stimulus. Some studies have analyzed the relationship between spontaneous pain and MRI findings.34950 Orsini et al.30 and Bertram et al.31 examined the relationship between provoked pain and MRI findings in relation to pain and disc displacement with and without reduction. Some authors reported pain to be significantly related to the MRI diagnosis of internal derangement,91832 while others reported no relationship.338
Moreover, some studies have examined the relationship between spontaneous and provoked pain and MRI findings.91826 Poor agreement was found between pain and internal derangement.1826 In this study, provoked pain on mouth opening was found to be correlated with internal derangement in TMD patients. However, spontaneous pain and provoked pain on manual palpation or mastication were not correlated with internal derangement.
The divergent results regarding the relationship between clinical findings and MRI could be attributed to the various criteria, study designs, and samples used. While some studies31530 examined symptomatic and asymptomatic individuals, others analyzed a wide spectrum of patients. This inconsistency resulted in a varied prevalence of disc displacement or internal derangement. Furthermore, the divergent results may also have been due to the techniques and criteria used to measure pain. Most studies included manual palpation in the clinical examination. Although manual palpation of the TMJ has acceptable reliability,51 the degree of TMJ pain is difficult to assess by this method. For this reason, an algometer52 is commonly used to measure pain thresholds in the orofacial region.5354 In this study, manual palpation, mouth opening, and mastication were used to measure provoked pain.
In general, pain intensity is measured via a visual analog scale,5052 pain scores,3031 or a verbal rating scale.55 McQuay and Moore56 demonstrated that several scales were reliable for measuring pain, and found visual analog scales and numerical rating scales to be the most commonly used. In this study, pain intensity was measured using a visual analog scale.
MRI may be indicated in patients with disc displacement without reduction. This condition is associated with a substantial history of limited mouth opening and reduced opening capacity. Adame et al.49 and Rammelsberg et al.57 reported data on opening capacity and attempted to correlate opening capacity with MRI findings. In this study, data regarding provoked pain on mouth opening were also obtained.
In conclusion, provoked pain on mouth opening was found to be correlated with internal derangement. However, provoked pain on palpation or mastication was not significantly related to internal derangement.
Further studies utilizing standardized diagnostic criteria and standardized methods are required.








 XML Download
XML Download