

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The implant position is one of the most important determinants of the long-term maintenance of implant esthetics and function.1 If an implant could be placed into the extraction socket at the same angulation as the that of the root inside the alveolar bone, the prosthetic crown would have an ideal position.23 Although the position of an implant should be based on future restoration plans, the placement of an implant axis in alignment with the crown is often limited by the morphology of the alveolar ridge.1
In addition to the root position in its alveolar socket, the thickness of the facial bone wall is also of crucial importance in selecting an appropriate treatment approach and determining the dimensions of the implant.45 In a previous study, the buccal bone wall of the anterior tooth was found to be very thin in most patients; therefore, the implant was positioned slightly on the palatal side to ensure sufficient buccal bone thickness.3 Especially in the esthetic zone, the facial bone wall is often thin and is predominantly composed of the bundle bone, such that its resorption results in a vertical reduction of the facial bony crest.6 Clinical guidelines suggest that a minimal buccal bone thickness of 1–2 mm is required to maintain the tissue architecture following tooth extraction and implant placement.7
The sagittal root position can have a significant impact on the occurrence of labial bone perforation, and cone-beam computed tomography (CBCT) images of the root position within the alveolar bone provide information that is useful for avoiding labial bone perforation.8 Therefore, preoperative diagnostic procedures are required to assess the risk factors for implant placement.49 Preoperative CBCT is now routine for implant placement, especially in the esthetic zone, both because of its accuracy and because of its convenience and low radiation dosage.10111213
The objective of this study was to measure the buccal bone thickness and angulation of the maxillary incisors and to analyze the correlation between these parameters and the root position in the alveolar bone using CBCT.
Materials and Methods
This study was approved by the Institutional Review Board of Pusan National University Dental Hospital. The subjects of this retrospective study were randomly selected from patients who visited Pusan National University Dental Hospital and underwent CBCT imaging between 2013 and 2014. Each image was examined to identify fully formed, intact, and healthy maxillary incisors for analysis. The CBCT data were excluded if any radiographically detectable caries, periapical pathology, alveolar bone loss of more than 4 mm from the cementoenamel junction, restoration, fracture, or history of orthodontic treatment was present. A total of 199 CBCT images met the inclusion criteria, resulting in a sample size of 398 maxillary central and lateral incisors. The patients comprised 100 males and 99 females, with a mean age of 28.3 years (range, 20–50 years).
All images used in this study were obtained using a PaX-Zenith 3D apparatus (Vatech Co., Hwaseong, Korea), with 5.7 mA, 110 kV, 24 s exposure time, 0.2 mm voxel size, and a field of view of 16×14 cm or 12×9 cm. CBCT data were saved in the Digital Imaging and Communications in Medicine format, and the images were analyzed using Ez3D Plus Professional CBCT software (Vatech Co., Hwaseong, Korea).
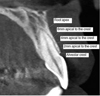
The arch form selector tool was centered at the middle of the arch in the axial plane. The root position, angulation, and buccal bone thickness were evaluated by viewing the cross-sectional images made at the midpoint of the tooth parallel to its long axis. The root position of the maxillary incisor in the alveolar bone was evaluated according to the position of the apex.14 The root position of the incisors was classified as follows: buccal type, the apical point of the incisor was within the buccal third of the alveolar bone and the root was closer to the buccal bone wall; middle type, the apical point of the incisor was within the middle third of the alveolar bone and the buccal and palatal bone walls were approximately equal in thickness; and palatal type, the apical point of the incisor was within the palatal third of the alveolar bone and the root was closer to the palatal bone wall (Fig. 1). The buccal type was further classified into subtypes I, II, and III. In subtype I, the incisor root was covered by the buccal bone wall and the bone thickness increased toward the apex. In subtype II, the incisor root was covered by a thinner buccal bone wall than found in subtype I and the bone thickness did not noticeably increase toward the apex that was covered by the bone tissue in the long axis of the tooth. In subtype III, the axis of the apex was angulated very buccally and the apex was not covered by the bone tissue in the long axis of the tooth (Fig. 2).
Furthermore, the angle between the long axis of the tooth and the long axis of the corresponding alveolar bone was determined. The long axis of the tooth was defined as the line through the lowest point of the crown to the highest point of the apex in the cross-sectional image (Fig. 3). The thickness of the buccal bone wall was assessed perpendicular to the long axis of the tooth at the following 5 locations: at the crest; 2, 4, and 6 mm apical to the crest; and at the root apex. If the root apex was located anterior to the natural contour of the maxillary alveolar buccal bone and the extremely thin bony wall belonged to buccal subtype III, a value of 0 mm was used to record the buccal bone thickness (Fig. 4).
All measurements were performed by a single examiner. The Kolmogorov-Smirnov test was used to determine the normality of the data. To estimate the intraexaminer deviations in the measurements, assessments of the maxillary incisors of 30 patients were performed twice. Two sets of measurements were carried out at different times on the same CBCT scans. The Wilcoxon signed-rank test was used to compare the numeric values of the duplicate measurements, and no significant differences were noted between the 2 sets of measurements. Moreover, no significant differences were observed between the measurements on the right and left sides. The Wilcoxon signed-rank test was used to compare the angulation and buccal bone thickness between the central and lateral incisors because the samples did not follow a normal distribution. The buccal bone thickness was presented as mean±standard deviation. In addition, the buccal bone thickness was grouped into the following categories for descriptive analysis: missing bone wall, bone thickness <1 mm, and bone thickness ≥1 mm. The Kruskal-Wallis test was conducted to compare the buccal bone thickness and angulation according to the root position. P values <.05 were considered to indicate statistical significance. The statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA).
Results
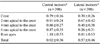
In this study, the root position within the alveolar bone was examined. A majority of the maxillary incisors were positioned more buccally within the alveolar bone. Among the buccal-type incisors, 64.3% of the central incisors were classified as subtype I and 67.6% of the lateral incisors were classified as subtype II. Only 2 lateral incisors (0.5%) were positioned more palatally (Table 1).
Furthermore, the angulation of the maxillary incisor within the alveolar bone was determined. The angulation of the maxillary lateral incisor was significantly greater than that of the central incisor (P<.05). The angulation of buccal subtype III was the greatest and that of the middle type was the lowest. A significant relationship between the root position within the alveolar bone and the angulation in the alveolar bone was found (P<.05; Table 2).
The mean thickness of the facial bone wall was 0.92 mm at the central incisors and 0.57 mm at the lateral incisors. The maxillary lateral incisors demonstrated a significantly thinner buccal bone thickness than the central incisors (P<.05). In the lateral incisors, the lowest bone thickness was observed 6 mm apical to the crest (Table 3).
A majority of the maxillary incisors exhibited a thin buccal bone wall (<1 mm). In addition, a thick buccal bone wall (≥1 mm) was found in 41.7% of the central incisors and 15.7% of the lateral incisors. The lowest percentage (4.5%) of thick walls was found 6 mm apical to the crest of the lateral incisors. At the root apex, the buccal bone was missing in 3.8% of the central incisors and 18.3% of the lateral incisors (Table 4).
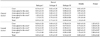
Table 5 shows the buccal bone thickness of the maxillary incisors according to sagittal root position. The buccal bone thickness of buccal subtypes II and III was significantly thinner than that of buccal subtype I at 4 mm, 6 mm, and the root apex of the central incisors and at 2 mm, 4 mm, 6 mm, and the root apex of the lateral incisors, respectively (P<.05). The buccal bone thickness gradually decreased apically at 2, 4, and 6 mm in buccal subtypes II and III.
Discussion
In this study, we investigated the root position in the alveolar bone, the sagittal angulation between the long axes of the teeth and their respective alveolar bone, and the buccal bone thickness of the maxillary incisors on CBCT images. Several studies have investigated the root position of the maxillary central incisors in the alveolar bone and have reported that the buccal type was the predominant incisor root position.25141516 In our study, the buccal type of root position was identified in more than 90% of cases and the palatal type was found in only 2 cases (5%) of the lateral incisors, similar to the results of previous reports.51416
We further classified the buccal type into 3 subtypes based on the thickness of the buccal bone wall at different root levels and the presence of an apical bone wall. Patients with buccal subtype I had an adequate buccal bone thickness and bone wall around the root. During immediate placement, the direction of placement more or less coincided with the long axis of the tooth.1417 In our study, buccal subtype I accounted for 64.3% of the central incisors and 8.0% of the lateral incisors. The buccal subtype II incisors had a thinner buccal bone wall than buccal subtype I, and immediate placement was more challenging than in patients with subtype I in such cases.14 The buccal subtype III teeth not only had a very thin buccal plate, but the axis of the root apex was also angulated very buccally, passing anterior to the natural contour of the maxillary alveolar bone.2 Therefore, patients with a subtype III root position may not be suitable for immediate placement.214 In this study, subtypes II and III were more frequent in the lateral incisors than in the central incisors.
The buccolingual inclination of the tooth was critical in determining the appropriate dental implant treatment approach and implant size.3 In this study, the angle between the long axis of the tooth and the long axis of the corresponding alveolar bone was less than 10° in buccal subtype I and the middle type. It may be relatively easy to insert implants into this kind of extraction socket. In our results, the angulation of buccal subtype III was the greatest, to the point that the implant position might be compromised.23
Numerous studies have revealed that a thin facial alveolar bone wall is usually present in the anterior maxilla.41518192021 Hence, in most situations, adjunctive bone augmentation has been recommended for immediate or early implant placement in the anterior esthetic zone.182223 The vertical resorption of the buccal crest was 3 times greater at sites with a thin buccal bone (<1 mm) than at sites with a thick buccal bone (≥1 mm).24 In this study, the buccal bone was thin (<1 mm) in 58.3% of the central incisors and 84.3% of the lateral incisors. Moreover, a statistically significant association was noted between the root position in its socket and the buccal bone thickness, and the buccal bone was significantly thinner in buccal subtypes II and III than in buccal subtype I. The buccal bone of the middle type was significantly thicker than that of buccal subtype I in the central incisors. However, there was no significant difference in buccal bone thickness between buccal subtype I and the middle type in the lateral incisors because the lateral incisors had thinner alveolar bones than the central incisors.
In conclusion, a majority of the maxillary incisors were positioned close to the buccal cortical plate and had a thin buccal bone wall. Significant relationships were noted between the root position in the alveolar bone, angulation in the alveolar bone, and buccal bone thickness. CBCT analyses of the buccal bone and sagittal root position are recommended for the selection of an appropriate treatment approach.






 XML Download
XML Download