

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Root surface area measurements are important for assessing orthodontic tooth movement.1 Optimal orthodontic force magnitudes are associated with the root surface area, particularly during orthodontic intrusion, because root surfaces are the regions that bear the highest amount of stress. Root surface area is also associated with tooth size, root morphology, root length, root diameter, root trunk width, and the number of roots.2
Three-dimensional (3D) information about dento-facial structures, including tooth roots, can be reconstructed from data acquired using cone-beam computed tomography (CBCT). CBCT units produce images with sub-millimeter resolution. The image accuracy of CBCT is higher than that of conventional computed tomography (CT) because the voxels of conventional CT are anisotropic, or cuboid, but the voxels of CBCT are isotropic, or cubic.3 The radiation exposure from CBCT is up to 10 times lower than that from conventional CT, yet CBCT offers a comparable image quality.4 In fact, CBCT produces considerably less scatter radiation than conventional CT does.4 Further, CBCT allows orthodontists to simultaneously, accurately, and easily measure the tooth size and the arch length discrepancy.
The membrane method is efficient for measuring the root surface area; however, tooth extraction is needed.1 The 3D laser scanning method using extracted teeth is more accurate, convenient, and time-saving. Recently, CBCT has also been used to obtain high-quality images of skeletal and dental structures because of its high spatial resolution. In the present study, we hypothesized that CBCT would be as efficient with respect to dental root surface area measurements as 3D laser scanning.
The objective of our investigation was to compare the root surface area measurements obtained from CBCT reconstruction before tooth extraction with those obtained from a 3D laser scanner after tooth extraction, and to evaluate the correlation between these 2 sets of measurements.
Materials and Methods
This study was approved by the Human Experimentation Committee of the Faculty of Dentistry, Chiang Mai University, Thailand (No. 19/2558). Informed consent was provided by all patients before we obtained the CBCT images. Thirty first premolars from 8 patients (2 males and 6 females; mean age, 18.0±3.4 years; range, 14.3–25.6 years) who required extractions for orthodontic treatment were selected. Pre-treatment CBCT images, prior to the first premolar extractions, were required for appropriate orthodontic treatment planning.
All CBCT images were obtained using a ProMax 3D (Planmeca Oy, Helsinki, Finland) CBCT unit. CBCT exposures were carried out at 84 kVp and 9 mA. The same exposure factors were used for obtaining all the images. The voxel size was 0.16 mm (high resolution), and the field of view was 8 cm×8 cm (diameter×height). The technical specifications of the Promax 3D CBCT are presented in Table 1. The maxillary and mandibular first premolars (samples) met the following inclusion criteria: 1) closed apices, 2) the absence of pathologic lesions in the root, and 3) continuous and clear cementoenamel junctions. Teeth were excluded for the following reasons: tooth or root damage during extraction, or the absence of radiographic images.
Root surface area measurements using CBCT before tooth extraction
CBCT images, stored as Digital Imaging and Communications in Medicine (DICOM) files, were imported into simulation software (Mimics version 15.01, Materialise, Leuven, Belgium) to convert the DICOM format to the stereolithography (STL) format. To reconstruct the areas of interest (first premolars) in the Mimics software, we first predefined the threshold value for the tooth region and then selected the “Region growing” function on the software toolbar. Once we selected the “Region growing” function, images of all the tooth regions were presented. Then, we selected only the areas of interest, which, for this study, were the first premolars. The details of the tooth root were refined by identifying the outer boundaries of the root area of each slice manually. To show the 3D model of the first premolar, we selected the “Calculate 3D” function. After producing the 3D model of the first premolar, we saved the file as an STL file; this file was then imported into 3-matic (version 7.01, Materialise) (Fig. 1). In 3-matic, we identified the cementoenamel junction based on its location and texture. Multiple points along the cementoenamel junction were created below the convex cervical third of the crown, where the smooth surface of the crown changed into the rough surface of the root. These points were also observed by changing the angulation between the crown and the root. These points were automatically connected by 3-matic, thereby drawing the line of the cementoenamel junction. The root surface area of each tooth was then automatically calculated (Fig. 2).
Root surface area measurements using a 3D laser scanner after tooth extraction
After extraction, the first premolar samples were cleaned using 100% sodium hypochlorite for 30 minutes, and all soft tissue and calculus were removed. All teeth were scanned, and the root surface area of each extracted tooth was calculated as follows. Step 1: Marking. Resin composite was used for marking the area above the cementoenamel junction (Fig. 3). Step 2: Scanning. The scanning range on the appropriate scope was set to cover the tooth specimen using a 3D laser scanner (D800 dental lab desktop scanner, 3Shape A/S, Copenhagen, Denmark) (Fig. 4). The D800 scanner with 2 5.0-megapixel cameras provided an accuracy as high as 15 µm.5 The collected data from each tooth were saved as STL files and imported into 3-matic. Step 3: Calculating the root surface area. The root surface area was measured using 3-matic.
In all the samples, the root surface areas were measured by a single examiner. The examiner repeated the root surface area measurements after a 4-week interval to determine the intraobserver reliability.
Statistical analysis
All data were tested for normality using the Shapiro-Wilk test. The total root surface areas were compared between the 3D laser scanner method and the CBCT reconstructions by the paired t-test. P values <.05 indicated statistical significance. Correlations between the 2 measurement methods were determined by calculating the Pearson correlation coefficient. The intraclass correlation coefficient (ICC) was used for assessing the intraobserver reliability of the 3D laser scanner and CBCT measurements.
Results
Root surface areas
The means and standard deviations of the root surface areas that were measured by the 3D laser scanner in the first and the second measurements were 229.24±42.43 mm2 and 229.38±41.49 mm2, respectively (P=.065). The means and standard deviations of the root surface areas that were measured by CBCT in the first and the second measurements were 229.74±41.57 mm2 and 230.49±42.57 mm2, respectively (P=.347). For both measurement methods, no statistically significant difference was observed between the 2 measurements (Table 2). The root surface area measurements obtained from CBCT reconstructions (230.11±41.97 mm2) were slightly higher than those obtained from the 3D laser scanner (229.31±42.46 mm2), but not significantly (P=.425) (Fig. 5).
Correlation between the 2 measurement methods
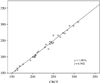
The correlation coefficient between the 2 measurement methods was 0.992 (Fig. 6). The statistical analysis showed that the ICC values obtained using the 3D laser scanner and CBCT were 1.000 and 0.990, respectively. Both 3D laser scanning and the CBCT measurements showed good ICC values.
Discussion
Confounding factors, such as gender, race, and patient age, across different studies might result in different root surface areas. On average, the root surface areas calculated by the weight conversion method are larger than those calculated by the membrane method or the division planimetric method.1 Several studies have shown that measurement methods such as the membrane method,6 division planimetry,7 and weight conversion8 have been used for measuring the root surface area in extracted teeth. Pan et al.9 evaluated the root surface area using 2-dimensional images, but making an absolute cut through the long axis of the tooth is extremely difficult. This technique might lead to failure to detecting apical or mid-root craters. Therefore, a quantitative measurement of the root surface area using CBCT seems to be beneficial for obtaining a 3D perspective. A previous study,10 which evaluated the root resorption by volumetric CBCT measurements after molar intrusion, demonstrated that CBCT was effective in evaluating volumetric root resorption, with no statistically significant difference between the laser scanning and the CBCT measurements. Gu et al.11 investigated the influence of root variations on the root surface area by using micro-computed tomography (micro-CT) of the extracted teeth and found that micro-CT was a precise technique for root surface area measurement. The quality and resolution of micro-CT images were better than those of CBCT images.1213 In our study, 3D laser scanning was considered to be a highly reliable and accurate technique because of the high resolution of the 3D laser scanner. The root surface area measurements obtained using 3D radiographic images and 3D laser scanning were compared to verify the accuracy of CBCT. Many factors can affect the accuracy of root surface area measurements made using CBCT. One such factor is the settings of the machine, which affect the quality of a CBCT image. Another factor is the manual editing process of outlining the root area. Furthermore using the CBCT measurement method, we found it difficult to identify the cementoenamel junction in the 3D radiographic images, and this difficulty might lead to differences in root surface area measurements. Some investigations1415 have suggested that the total amount of radiation received from CBCT is minimal, approximately 20% of that of conventional CT and equivalent to that of a full-mouth periapical radiographic exposure. However, patient selection for CBCT should carefully consider the amount of radiation and should follow the principles of as low as reasonably achievable. A drawback of the 3D laser scanner method is the need for tooth extraction prior to root surface area measurements. Accordingly, for the root surface area measurement of non-extracted teeth, CBCT should be considered as an appropriate method.
In summary, in this paper, we presented a novel CBCT approach for measuring the root surface area. Our investigation revealed that CBCT was efficient for dental root surface area measurements.







 XML Download
XML Download