

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Nasal respiration and its relationship with the growth and development of the craniofacial structures has been extensively studied due to its functional concern to pediatricians, orthodontists, otorhinolaryngologists, allergists, and speech therapists.1
The pharyngeal airway is an anatomical space divided into the nasopharynx, oropharynx, and laryngeal pharynx. Individuals with impaired nasopharyngeal airways may tend to exhibit mouth breathing due to the enlargement of the adenoid tissue.23 Associated factors may also induce mouth breathing, among which are constriction of the nasal passage, a narrowed or obstructed nasopharynx, hypertrophic nasal membranes, enlarged turbinates, hypertrophic palatine or pharyngeal tonsils, nasal septal deviation, choanal atresia, and pathology in the nose or nasopharynx.4 Upper airway size can also be affected by posture, gender, age, obesity, and body mass index.5
It is generally accepted that the upper airway structures play a significant role in the development of the craniofacial complex.678 Narrowed pharyngeal airway dimensions can cause deficient breathing, resulting in a reduction of growth hormone levels in growing children and obstructive sleep apnoea in adults.910 Patients suffering from obstructive sleep apnoea and an associated reduction in the pharyngeal airway tend to have features typical of angle class II subjects,11 characterised by a short and retrognathic mandible12 and sagittal discrepancy.13
Skeletal class II malocclusions are characterised by a retrusion of the mandible, protrusion of the maxilla, or a combination of both.14 The correction of a skeletal class II malocclusion is therefore based on 3 basic interventions related to the patient's growth: growth modification, dental camouflage, or orthognathic surgery.1516
It has been reported that breathing disorders can cause maxillofacial growth problems, vertical facial development, and a skeletal class II malocclusion, and that they can lead to a posterior crossbite.17 In a recent study by Kim et al., children with skeletal class II malocclusions and retrusive mandibles had smaller pharyngeal airway dimensions than children with skeletal class I malocclusions.18
Therefore, we hypothesised that deficient mandibular growth might be a factor in reduced oropharyngeal airway dimensions and related impaired respiratory function. Accordingly, the purpose of the present study was to evaluate the nasopharyngeal and oropharyngeal dimensions in skeletal class II subgroups, that is, individuals with skeletal class II, division 1 and skeletal class II, division 2 patterns with retrusive mandibles during the pre-peak, peak, and post-peak growth periods for comparison with a skeletal class I control group.
Materials and Methods
This retrospective cross-sectional study was based on the pre-treatment lateral cephalograms of 124 individuals selected from the archives of the Ankara University Faculty of Dentistry Department of Orthodontics (Table 1) according to the Ethics Committee of the university. In order to classify orthodontic malocclusions, the pre-treatment study models showing canine and molar relationships, overjet, overbite, and lateral cephalograms were examined.
The subjects were classified into 3 growth periods: the pre-peak, peak, and post-peak growth periods, using handwrist maturation stages as determined by the Greulich-Pyle method.19 The pre-peak growth period was defined as the period when the epiphysis of the proximal phalanx of the index finger was of the same width as the diaphysis (PP2), when the epiphysis of the middle phalanx of the middle finger was of the same width as the diaphysis (Mp3), and by the first mineralization of the ulnar sesamoid bone (S). The peak growth period was defined as the period when the diaphysis was covered by the capshaped epiphysis at the middle phalanx of the third finger (Mp3cap). The post-peak growth period was defined as the period when the following outcomes were identified: the visible union of the epiphysis and diaphysis at the distal phalanx of the middle finger (Dp3u), the visible union of the epiphysis and diaphysis at the proximal phalanx of the middle finger (PP3u), the visible union of the epiphysis and diaphysis at the middle phalanx of the middle finger (Mp3u), and the complete union of the epiphysis and diaphysis of the radius (Ru). The hand-wrist radiography samples for each group are shown in Figure 1, while cephalometric radiography samples are shown in Figure 2.
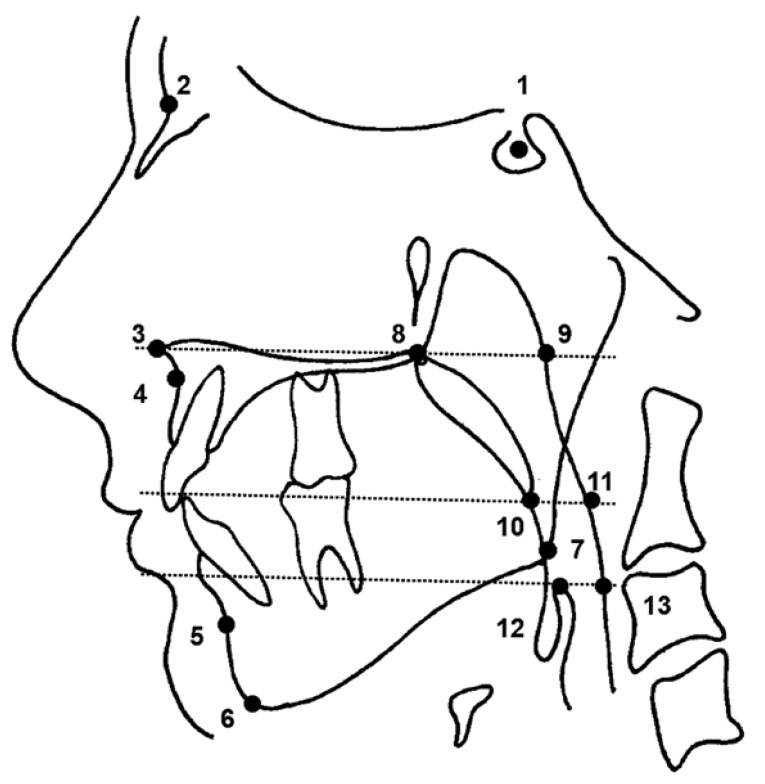
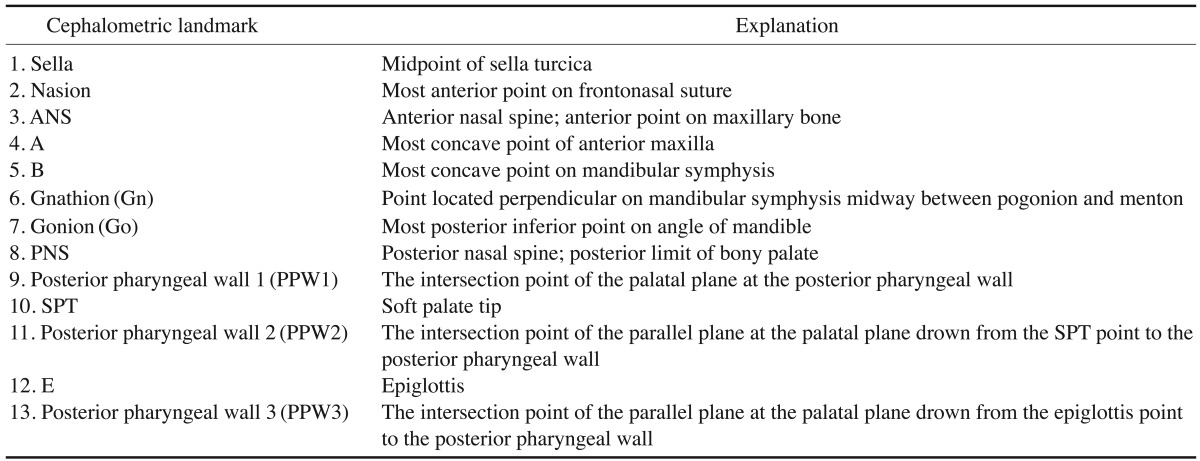
All lateral cephalometric radiographs had been taken using conventional methods, by the same radiographer, with the Frankfort horizontal plane parallel to the floor. The magnification ratio of the cephalometric machine was 1.1. The cephalometric reference points (Fig. 3) and the explanations for them are shown in Table 2.
Using these cephalometric landmarks, 4 angular measurements (the gonion-gnathion/sella-nasion [GoGn/SN], sella-nasion-A-point [SNA], sella-nasion-B-point [SNB], and A-point-nasion-B-point [ANB] angles), 4 linear measurements (soft palate length [SPL]: the distance between the posterior nasal spine [PNS] and soft palate tip [SPT]; nasopharyngeal airway space [NAS]: the distance between PNS and the posterior pharyngeal wall 1 [PPW1]; upper oropharyngeal airway space [OAS]: the distance between SPT and the posterior pharyngeal wall 2 [PPW2]; lower oropharyngeal airway space/oropharyngeal airway space 2 [OAS2]: the distance between the epiglottis [E] and the posterior pharyngeal wall 3 [PPW3]), and 4 proportional measurements (anterior nasal spine [ANS]-PNS/SPT, SPL/NAS, SPL/OAS, SPL/OAS2) were identified in this study. Lateral cephalograms were traced and reference points were marked on an acetate paper by the observer. Then, the anatomic landmarks were transferred to a computer programme (Purpose on Request Digitizer Input Output System, Institute of Orthodontic Computer Science, Randers NV, Denmark) using a digitizer for calculating the measurements.
In order to estimate the reliability of the measurements, repeated measurements of 30 cases were conducted after an interval of 1 month by the same observer and intraclass correlation coefficients were calculated. All measurements had high repeatability coefficients (max=0.99, min=0.92), thus confirming the reliability of the measurements.
The means and standard deviations of the parameters were calculated for the ratio and interval data, following a normal distribution. The statistical analysis of the study was performed by using Repeated Measurements Analysis of Variance and the Duncan test. Repeated Measurements Analysis of Variance was used to compare intragroup and intergroup cephalometric measurements for each growth period. To evaluate the interaction among growth periods and study groups, growth-group interactions were analyzed. The values are presented in the form of mean±standard deviation.
Results
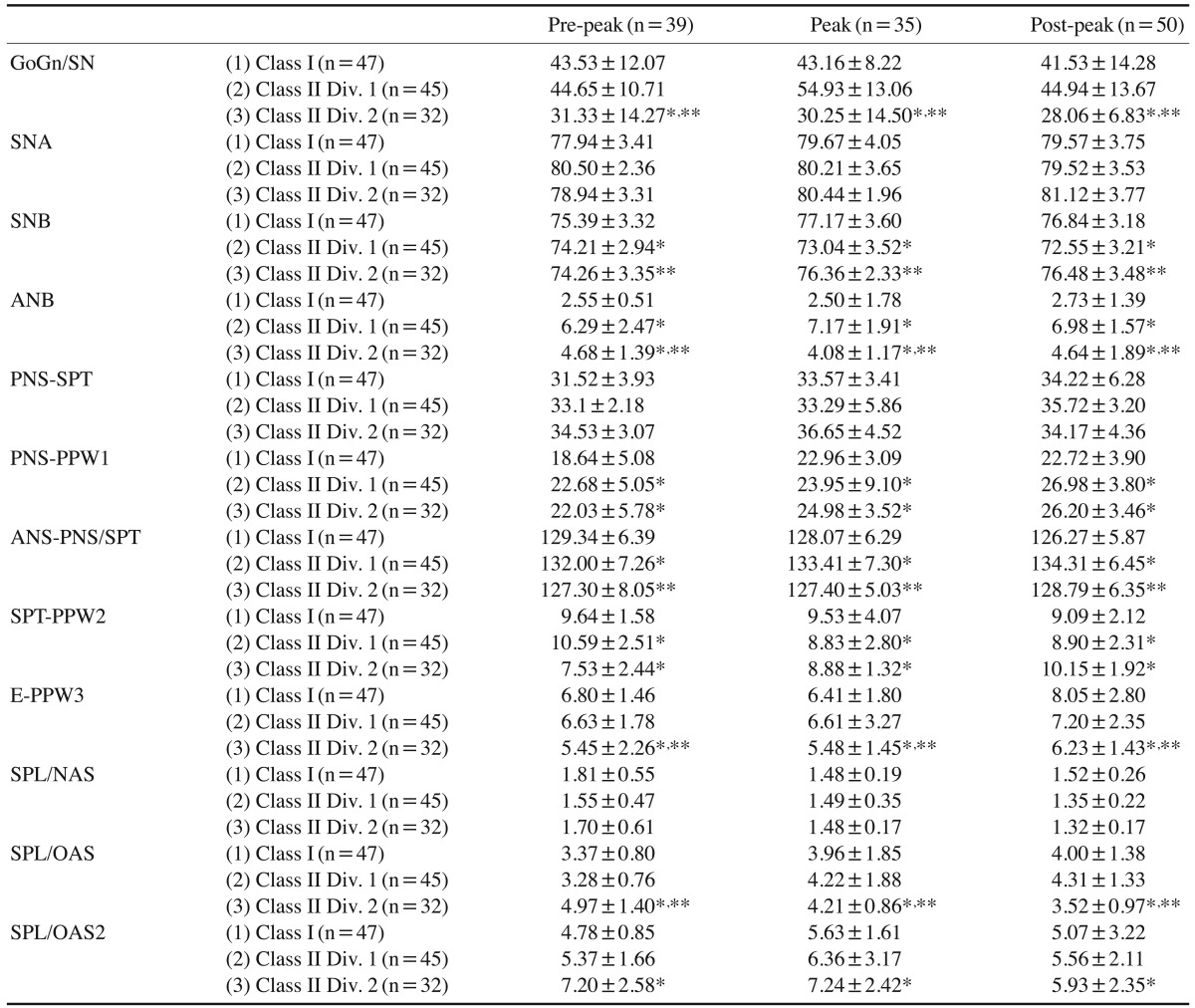
Table 3 shows the comparison of cephalometric and pharyngeal airway measurements in class I, class II, division 1, and class II, division 2 groups, including interactions. Accordingly, statistically significant differences were found between the class II, division 2 group and other groups for the GoGn/SN angle, which showed a decrease in vertical facial dimensions in this group. The SNB angle was statistically different among the groups (p<.05), while the ANB angle was significantly different for all 3 groups (p<.05) (Table 3). The nasopharyngeal airway space (PNS-PPW1) showed a linear increase in the skeletal class II groups at a significance level of p<.05.
The OAS2 measurement showed a statistically significant difference between the groups (p<.05), with the smallest dimension in the class II, division 2 group (Table 3), which should be considered in differential diagnosis of skeletal class II cases. However, the SPL/NAS ratio did not show a significant difference among the groups (Table 3), while showing an increase during puberty.
The SPL/OAS ratio was statistically different among class I, class II, division 1, and class II, division 2 groups in the pre-peak period (Table 3). The SPL/OAS2 ratio was only different between the class I and class II, division 2 groups (Table 3).
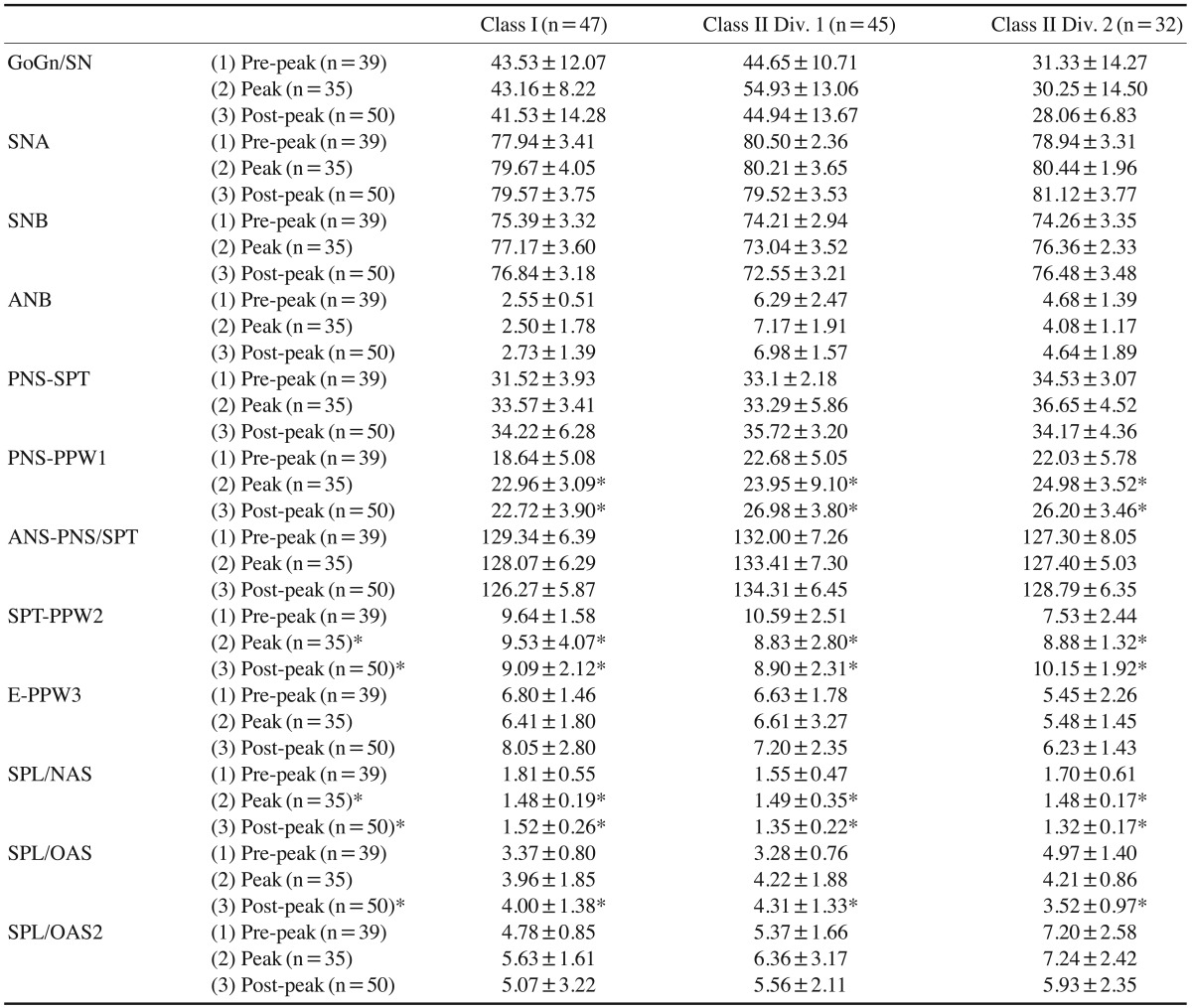
Table 4 indicates the comparative differences of the parameters according to the growth periods, including interactions. Accordingly, there were no significant differences for GoGn/SN, SNA, SNB, and ANB angles during prepeak, peak, and post-peak growth periods.
The NAS measurement increased during growth in class II, division 1 and division 2 groups; however, while it showed an increase from pre-peak to peak period in the class I group, a small decrease occurred in the post-peak phase, while it showed a minimal increase in the control group. The ANS-PNS/SPT angle decreased only in the control group, and increased in the skeletal class II groups (p<.05). The OAS measurement decreased in the control group during growth and showed a linear increase in the class II, division 2 group, which can be interpreted as the compensation of mandibular retrusion that impairs the lower pharyngeal airway. The SPL/OAS2 ratio showed an increase between the pre-peak and peak growth periods and thereafter showed a decrease (Table 4).
The interaction plot for the nasopharyngeal airway space (PNS-PPW1) showed a statistically significant difference among the groups and the growth periods (p<.05).
The interaction among the growth periods and study groups was statistically significant regarding the upper oropharyngeal airway space (OAS) measurement (p<0.05), which demonstrated that the change in the OAS dimension is statistically different among the groups during growth (Table 4).
The SPL/OAS ratio showed a statistically significant difference during the pubertal growth period, pre-peak to post-peak, in the skeletal class II groups, which might be clinically important for identifying the variation in the SPL/OAS ratio in the aforementioned groups.
Discussion
The current study evaluated the nasopharyngeal and oropharyngeal dimensions of individuals with mandibular retrognathism and compared the results with a skeletal class I control group during different growth periods; accordingly, skeletal and airway measurements were performed on cephalometric radiographs that were taken before treatment. It has been accepted that measurements on a 2-dimensional cephalometric radiograph cannot reveal the transverse dimensions of the airway. However, it has been reported that cephalometry is easy to use, economical, and can provide definite and quantitative information about the soft palate and nasopharynx.2021 Aboudara et al.22 showed that there was a significant positive relationship between nasopharyngeal airway size on cephalometric radiographs and its true volumetric size as determined by cone beam computed tomography in adolescents. Lateral cephalograms are still the major evaluation tool for upper airway research, despite their disadvantages.23 However, lateral cephalometric radiographs should be taken in natural head posture to measure nasopharyngeal airway size dimensions precisely, because head position may influence upper airway dimensions, a possibility that has previously been proposed by many authors.2425
It has been previously reported that nasopharyngeal dimensions continue to grow rapidly until the age of 13, after which deceleration occurs until adulthood.62627 On the one hand, similar to other findings in the literature, the present study clearly showed that PNS-PPW1 and the lower oropharyngeal airway space (E-PPW3) exhibited an increase during growth in all malocclusion groups. However, the upper oropharyngeal airway space (SPT-PPW2) increased only among class II, division 2 patients during growth. On the other hand, a statistically significant difference in the upper oropharyngeal airway among groups and growth periods was found, showing an association of SPT-PPW2 with craniofacial growth pattern and malocclusion type. This is at variance with the findings of previous studies.26272829
Zhong et al.30 found that the sagittal skeletal pattern may be a contributory factor in variations in the inferior part of the upper airway. Sosa et al.31 found no relationship between the nasopharyngeal area and class I or class II, division 1 malocclusions. Similarly, Wenzel et al.32 reported no correlation between airway size and mandibular morphology. However, Ceylan and Oktay29 stated that pharyngeal structures were not affected by the ANB angle, while a significant difference was found in the oropharyngeal area between class I and class III, and between class II and class III.
Concerning the malocclusion type versus pharyngeal airway size studies in the literature, De Freitas et al.33 compared the upper and lower pharyngeal widths in 80 patients with untreated class I and class II malocclusions. They showed that the upper pharyngeal width in subjects with class I and class II malocclusions and vertical growth patterns was statistically significantly narrower than in subjects with normal growth pattern. It was found that malocclusion type did not influence upper pharyngeal airway width and malocclusion type and growth pattern do not influence lower pharyngeal airway width.33 Alternatively, Alves et al.34 performed a 3-dimensional cephalometric study of upper airway space in skeletal class II and III healthy patients. Their results revealed that the majority of the airway measurements were not affected by the type of malocclusion. However, they reported that the evaluation of upper airway space should be an integral part of diagnosis and treatment planning to achieve functional balance and stability of the results.34 Later, Memon et al.35 performed a study on the cephalograms of 360 orthodontic patients and found that sagittal malocclusion type did not influence upper pharyngeal width.
On the contrary, Kerr36 reported that class II malocclusion subjects showed smaller nasopharyngeal dimensions than class I and normal subjects. El and Palomo23 evaluated the nasal passage and oropharyngeal volumes of patients with different dentofacial skeletal patterns. The oropharyngeal airway volumes of class II patients were smaller than those of class I and class III patients. Mandibular position with respect to cranial base was noted to have an effect on the oropharyngeal airway volume. Similarly, Kerr36 and Keçik37 found that class II malocclusion patients showed smaller nasopharyngeal dimensions than class I subjects. Subsequently, the present study found a significant difference in nasopharyngeal airway space and upper oropharyngeal airway space between class I and class II subgroups. Moreover, the lower oropharyngeal airway space showed a statistically significant increase in the class I group compared with the class II, division 2 group. Correspondingly, Grauer et al.38 assessed the differences in airway shape and volume among subjects with various facial patterns. Cone-beam computed tomography records of 62 non-growing patients were used to evaluate the pharyngeal airway volume and shape. A statistically significant relationship was found between the volume of the inferior component of the airway and the anteroposterior jaw relationship, and between airway volume along with the size of the face and gender.
In the present study, the nasopharyngeal airway space showed the smallest dimensions at the pre-pubertal growth stage for class I and class II subgroups (Table 3). The smallest dimension of OAS2 was recorded in the class II, division 2 group; hence, the oropharyngeal airway dimension should be carefully considered for treatment timing. If there is no finding of upper nasopharyngeal airway pathology related to oversized adenoids or tonsils, or chronic respiratory problems, early correction of a skeletal class II, division 2 malocclusion might eliminate the possibility of having disturbed respiratory function during sleep, such as snoring.39
However, the SPL/NAS ratio, which plays an indispensable role in velopharyngeal function, did not show a statistically significant difference among the groups (Table 3), while the differences were statistically significant among the different stages of the growth process (Table 4).
In conclusion, the naso-oropharyngeal airway dimensions showed a statistically significant difference among the class II, division 1; class II, division 2; and the class I control groups during the different growth periods.
With an appropriate treatment plan considering nasooropharyngeal dimension differences, an improvement in the skeletal relationship may benefit naso-oropharyngeal airway dimensions, as well as improve the facial profile and dentoalveolar relationships.



 XML Download
XML Download