

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Oculo-auriculo-vertebral spectrum (OAVS) represents a collection of anomalies due to the dysmorphogenesis of the first and second branchial arches, and incorporates Goldenhar syndrome and hemifacial microsomia.123 It has been suggested that these two conditions represent different manifestations of a similar error in morphogenesis.4 Although the etiology of this spectrum is uncertain, animal models have suggested that OAVS is due to a disruption in the vascular supply to the first and second branchial arches.5 The most prominent features of the spectrum related to the head and neck are aural, oral, and mandibular anomalies including, but not limited to, facial asymmetry, cleft lip, cleft palate, microtia, accessory tragus, epibulbar dermoid, parotid gland agenesis, and dental malocclusion.6 Cosmetic and reconstructive surgery, including soft tissue implants or grafts, is often indicated to address these facial abnormalities.
An implant is defined as “an object or material inserted or grafted into the body for prosthetic, therapeutic, diagnostic, or experimental purposes,” and a graft as “any tissue or organ [used] for implantation or transplantation.” 7 Facial implant materials that have been used for soft tissue contouring include silicon rubber (Silastic™), expanded polytetrafluoroethylene (Gore-Tex®), polytetrafluoroethylene (Teflon™), porous polyethylene (Medpor®), and hydroxyapatite.8 Among the most successful and commonly used grafts in maxillofacial reconstruction are autogenous costochondral grafts (CCGs), which were introduced by Gillies in 1920.9101112131415
CCGs are most commonly used for mandibular condyle and ramus reconstruction, due to their biological and morphological resemblance to the mandibular condyle. The growth potential of these grafts is substantial, and can be unpredictable.9 Unfavorable growth, fractures, and reankylosis of the mandibular condyle are well-documented complications of this type of graft.9 The overgrowth can be attributed to the primary cartilage in CCGs, which acts as a growth center. In addition, the size of the cartilaginous cap, degree of physiologic function, and hormonal influences may play a role in the incidence and degree of overgrowth. It is uncertain whether these grafts grow as a result of inherent or adaptive growth, or a combination of both processes.9 Autogenous CCGs have also been used as cosmetic grafts. They are subject to the same patterns of growth and overgrowth.
We present the case of a cosmetic autogenous CCG that posed a diagnostic challenge both radiographically and histopathologically. To our knowledge, the imaging features of such grafts on cone-beam computed tomography (CBCT) have not been documented in the literature.
Case Report
An 81-year-old female with OAVS presented to a general dentist for a dental implant consultation. Her medical history was remarkable for an epibulbar dermoid and previous grafting of an anterior mandibular defect at the age of 16. The patient was asymptomatic. After a routine examination, the patient was referred to an oral and maxillofacial surgeon for implant treatment planning. The surgeon requested a maxillofacial CBCT scan extending from the level of the nasal fossa through the inferior border of the mandible, and from the anterior border of one ramus to the anterior border of the contralateral ramus.
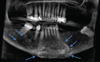
Upon radiographic examination, the bilateral paramedian area of the mandible appeared abnormally heterogeneous with a poorly defined border on the right. The mandibular canals anterior to the right second molar and the left mental foramen were untraceable (Fig. 1). Multiplanar reconstructions revealed a large, heterogeneous, expansile entity of mixed density along the facial side of the mandible, extending from the mandibular left premolar area to the mesial aspect of the mandibular right third molar, and from the level of the root apices through the inferior border of the mandible. Thinning of the lingual cortical plate was noted in some areas (Fig. 2). Effacement of the facial cortical plate without an effect on the neighboring teeth was observed (Fig. 3). Three-dimensional volume rendering depicted the considerable size of the entity in question (Fig. 4). A cartilaginous neoplasm could not be ruled out based on CBCT imaging and an incisional osseous biopsy was therefore performed.
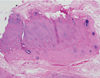
Hematoxylin and eosin-stained slides prepared after formalin fixation and decalcification were reviewed (Fig. 5). Multiple fragments of benign and hypocellular cartilage with adherent fibrous tissue were present. No osseous-cartilaginous integration could be detected from the limited sample. The appearance was consistent with normal cartilage.
Discussion
Growth or overgrowth is a recognized sequela of CCGs. Almost all patients that seek corrective surgery following CCG overgrowth in the mandibular body or condyle present with facial asymmetry. This happens even when the grafts are placed bilaterally due to their unpredictable growth potential. For a definitive diagnosis to be made, radiographic examination followed by a histopathological evaluation is indicated.9
Most of the published cases of CCG overgrowth in the mandible were described radiographically using panoramic images and/or multi-detector computed tomography (MDCT).10111415161718 Yang et al.9 reviewed 68 cases of CCG overgrowth in the maxillofacial region. The authors described a case of overgrowth of a CCG that replaced the right mandibular body using panoramic, lateral cephalometric, and posteroanterior skull radiographs, and MDCT. None of the radiographs demonstrated asymmetry due to the inherent limitations of this imaging modality. MDCT allowed better visualization of the facial deformity and chin deviation in all dimensions.9 The advantage of the 3-dimensional visualization of such complex cases using MDCT is indisputable. However, plain radiography is still commonly used due to its availability, low cost, and reduced patient exposure to ionizing radiation. Raustia et al.17 analyzed 11 cases of CCGs replacing the mandibular condyles using MDCT. The authors reported 4 cases that demonstrated low-attenuation grafts with occasional foci of high attenuation, clear borders between the graft and host bone, and lateral and superior rims of ossification using MDCT. The follow-up period of these cases ranged from 5 months to 8 years. A clear border was only seen in the case in which only 5 months had elapsed since surgery. Fukuta et al.16 published a case of recurrent overgrowth of a CCG placed for hemimandibular reconstruction using panoramic images, MDCT, and a nuclear medicine bone scan. These images were of poor quality, but the authors noted the deviation of the mandible on MDCT on 2 occasions (before each corrective operation) and increased uptake of the radionuclide by the graft on the third day after surgery. This profound growth potential may have been due to the patient's young age (2 years old). Similarly, Samman et al.18 demonstrated an increase in isotope uptake by the graft using technetium scintigraphy, supporting the theory that CCGs have an inherent growth potential. Kaban et al.11 described the incorporation and calcification of a CCG replacing the mandibular condyle, and ultimately resembling a normal condyle upon periodic follow-up. Unfortunately, the quality of the images was poor in the previous articles, which made us unable to evaluate the imaging findings.
Eckardt et al.10 described a case of CCG reconstruction after hemimandibulectomy in which follow-up was performed at regular intervals, up to 6 years after surgery, using panoramic images. The authors used linear and angular measurements to calculate the ratio between the operated and unoperated side to evaluate overgrowth versus growth retardation. Although this approach is inaccurate, as panoramic images are prone to positioning errors and unpredictable distortion between successive images and within the same image;19 significant growth of the CCG along the vertical dimension was evident. Ko et al.13 accurately used landmarks on lateral and posteroanterior cephalometric radiographs to assess CCG growth. The authors noted that the follow-up period was critical when evaluating overgrowth; the longer the follow-up period, the more growth they found in their sample. They did not display any radiographs. Jang et al.20 described the case of a CCG extending from the angle of the mandible and replacing the condyle using CT. The graft appeared stable with no signs of resorption or overgrowth at 10 months after surgery. This may have been due to the short follow-up period.
Schatz and Ginat8 pointed out that autografts have the disadvantage of resorption hindering their cosmetic effect. The authors demonstrated a low-attenuation cartilage graft with a peripheral rim of ossification using an axial MDCT image. Karacaoğlan et al.21 also demonstrated that cartilage grafts had a tendency to undergo resorption, using magnetic resonance imaging (MRI) after a 12-month follow-up period to assess the degree of resorption. The majority of the grafts had a low signal with a few foci of high signal near the soft tissue periphery on follow-up imaging.
No article in the literature described similar growth or changes in synthetic cosmetic implants in the soft tissue. This is attributed to the fact that they lack growth potential. However; cosmetic implants, like autogenous grafts, can become incorporated into the underlying bone. Other complications associated with cosmetic implants include migration, extrusion, erosion, and foreign bone reaction.8
With the increased use of radiographic imaging to diagnose and treat a variety of dental and medical conditions, there is an increased likelihood of incidental findings, such as implants that were not expected based on the patient's history. A history of implants for cosmetic purposes may not be elicited because the patient may not feel that they are important to the issue being discussed. Although most implants and grafts will present as benign-looking entities within the soft tissue that can easily be interpreted as such, some may present as unusual entities that may mimic a more serious disease, such as a benign or malignant neoplasm. The current case was such a situation, in which a CCG appeared suspicious.
The common management of facial defects in OAVS includes reconstructive surgery, often using implants or grafts to improve patients' cosmetic appearance. We present the case of an incidentally found cosmetic graft. According to the patient, an autogenous rib graft was harvested and sectioned to augment the mandibular symphysis. On imaging, no surgical hardware was identified. Attempts to recover previous medical and surgical notes were unsuccessful, as the surgeon who performed the procedure in 1950 was deceased. The exact surgical technique used was unclear; however, the graft had maintained its proper anatomical location and aesthetic shape for over 65 years. The most probable surgical technique may have involved the surgeon dicing the osteocartilage into multiple pieces and creating a tunnel between the mandibular periosteum and overlying mucosa to hold the diced cartilage graft in place during the healing period.21 To our knowledge, this is the last published case of an anterior mandibular costochondral graft. No case with long-term follow-up has been published and a review of the literature concerning imaging related to cosmetic facial grafts did not identify any similar cases.
Clinical correlations, imaging, and histology were essential to render a final diagnosis of costochondral graft material. The histopathology suggested a benign cartilaginous process; however, the anterior mandible is a rare site for benign cartilaginous neoplasms, and without proper clinical and radiographic correlations the lesion could have been misdiagnosed.
Other possibilities in the histological differential diagnosis included the cartilaginous cap of an osteochondroma. However, mandibular osteochondromas have almost exclusively been reported in the condyle.22 The characteristic imaging findings of an osteochondroma, involving a pedunculated or sessile bony cortical mass continuous with the underlying bone, were absent.
Facial implants and grafts are found incidentally in many CBCT studies performed for dental treatment. A thorough knowledge of their normal appearance is important in order to recognize what is abnormal. Based on imaging alone, chondrosarcoma was initially considered due to the speckled diffuse flocculent calcification and the infiltration into adjacent normal bone. Chondrosarcomas occur where cartilaginous tissues may be present and may occasionally occur in the symphyseal region.23
Schatz and Ginat8 discussed the imaging appearance of these augmentation materials using CT and MRI. Chin augmentation materials such as hydroxyapatite, silicone implants, and cartilage grafts have been described. The authors concluded that cartilage grafts appear to have a soft tissue density that “may form a rim of calcification or ossification.”8 Our case involved a more diffuse calcification pattern, which may have been due to the longer follow-up period.
Implants or grafts may be incidental findings on radiographic images made for unrelated purposes. Although most are well defined and radiographically homogeneous, being of relatively inert non-biological material, immune reactions to some may stimulate alterations in the appearance of surrounding tissues. Biological implants may undergo growth and differentiation, causing their appearance to mimic neoplastic lesions.
We present the case of a costochondral graft in the soft tissue anterior and facial to the mandible, with changes mimicking a cartilaginous neoplasm. In light of the fact that chondrosarcomas are known to occur in the anterior rib cage, an evaluation of random growth is warranted when a CCG is used for reconstructive surgery. A vascularized graft is thought to be more controlled in growth than a nonvascularized graft. This is the first case to report the CBCT imaging features of a long-standing graft in the anterior mandible.



 XML Download
XML Download